A number of states have decided to opt out of expanding Medicaid, despite the fact that for the first three years, 100% of the costs of the Medicaid expansion would be covered by the Federal government. This has a number of fiscal, health and mortality implications.
According to Opting Out Of Medicaid Expansion: The Health And Financial Impacts, by Sam Dickman, David Himmelstein, Danny McCormick, and Steffie Woolhandler, the implication of 25 states opting out of the Medicaid expansion (the incremental costs of which would be covered 100% by the Federal government in the first three years, and 90% as of 2020) would be increased mortality levels of between 7,115 to 17,104, per annum. Even assuming no increase in the number of people who would be covered under the expansion over time (so for instance if population were to stay constant), the cumulative increased mortality count relative to full Medicaid expansion becomes noticeable quickly.
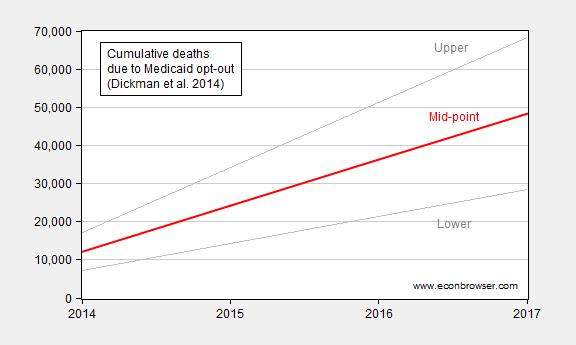
Figure 1: Linear extrapolation of per annum enhanced mortality levels due to Medicaid expansion opt-out, lower and upper (gray lines), and midpoint (red). Source: Sam Dickman, David Himmelstein, Danny McCormick, and Steffie Woolhandler, “Opting Out Of Medicaid Expansion: The Health And Financial Impacts,” Health Affairs Blog (Jan 30, 2014), Exhibit 3, and author’s calculations.
There is nothing mysterious about how these estimates are obtained. It’s essentially:
D = U × Rc × Rm
Where D is the incremental mortalities due to opting out of Medicaid expansion, U is total number of uncovered pre-expansion, Rc is the ratio of uncovered who would be covered by the Medicaid expansion, and Rm is the ratio of the covered who would live that in the absence of coverage would die. Hence, the mechanics are fairly straightforward. Rc is estimated at 7.8 million by Dickman et al. Rc, the ratio that would be covered by expansion, seems fairly straightforward. Urban Institute estimates 5.8 million. There has been some debate over Rm, with individuals from the NC/AEI/Mercatus and Manhattan Institute taking issue with the upper estimate. [1].
Governments in the 25 states indicated in dark blue have decided not to expand Medicaid.
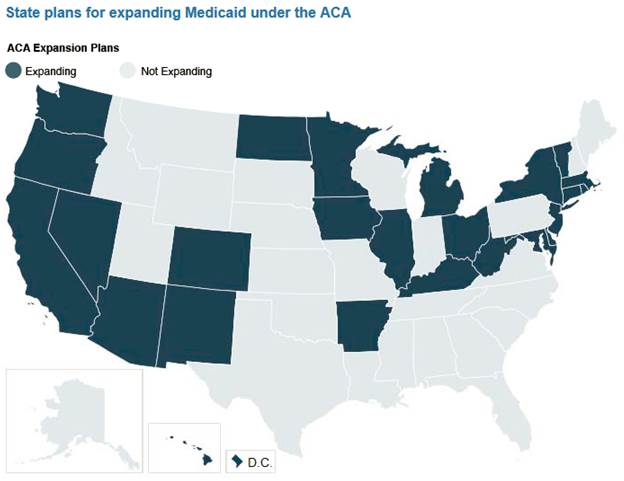
Figure from Urban Institute.
Florida and Texas alone account for nearly 3.3 million of the total 7.8 million of individuals that would be covered were Medicaid to be expanded in the opt-out states. That means mid-point estimates for incremental deaths per annum are 1,700 and 2,450, respectively.
As economists, we want to cast choices in terms of benefit-cost ratios. Doing so in this case, however, does not change the point that it makes sense from an individual state finance perspective, to have expanded Medicaid. CBO has estimated that over the next ten years, the Federal government will pick up over 95% of total costs [2] Indeed, with Federal transfers declining, and state spending for uncompensated care increasing by at least $1 billion in 2016 (estimate is for 14 states opting out),[3] the Medicaid opt out can only be interpreted as being driven by non-economic motives.
think you erred on this: “Governments in the 25 states indicated in dark blue have decided not to expand Medicaid.” (drop the not)
rjs: Apologies, you are correct. Thank you for pointing that out. Fixed now.
Menzie
This is the second “economic” post in recent memory that is beneath you as an economist, the other being your GDP numbers before and after WWII. What is in common with both of those post is your acceptance of numbers without any written thought to what they mean. And anyone can do that, read the following written in the style of Menzie Chinn.
The implication, intent, and mandate of ACA is straight forward, by the law everyone must purchase health insurance. And because of the highly limited availability of medical access for those on Medicaid, as compared to the other plans made available through ACA; which means that the implication of 25 states opting
out ofinto the Medicaid expansion (the incremental costs of which would be covered 100% by the Federal government in the first three years, and 90% as of 2020) will result in a number of people with inferior coverage. Even assuming no increase in the number of people who would be covered under the expansion over time (so for instance if population were to stay constant), the cumulative increased mortality count relative to full Medicaid expansion becomes noticeable quickly.There is nothing mysterious about how these estimates are obtained. It’s essentially:
D = U × Rc × Rm
Where D is the incremental mortalities due to opting
out ofinto Medicaid expansion, U is total number of uncovered pre-expansion, Rc is the ratio of uncovered who would be covered by the Medicaid expansion, and Rm is the ratio of the covered by the mandated purchase of other ACA plans who would live that in the absence of forced Medicaid coverage would die.I now refer you to the the above Figure 1 relabeled as Cumulative deaths due to Medicaid opt-
outinAs with many of your post, Menzie, it “can only be interpreted as being driven by non-economic motives.”
And as the political season is quickly coming, I expect many more to come.
Ed
One minor typo: “stated indicated in dark blue have decided not to expand Medicaid.” The opposite is true, according to the legend.
JTapp: Apologies, you are correct. Thank you for pointing that out. Fixed now.
It appears that the “nothing mysterious” part is highly dependent on the accuracy of Rm… and alternative sources of care available. Remember: GIGO.
Bruce Hall: Well, that’s why I included upper/lower/midpoint estimates. But I take your point, GIGO, e.g. for a prominent example [1]
Menzie, I appreciate the fact that you put in upper and lower estimates, but those are still dependent on a valid Rm. With regard to the “prominent example”, there are enough comments on that post that I don’t have to go into it.
Regardless, there is value in providing assistance to people who absolutely cannot afford or find health care. I’m not convinced that the dynamics of the ACA/expanded Medicaid is the way to do that… and for many people, the jury is still out on that. A major element of unaffordable health care is the cost the doctors incur simply to do business. The new electronic records requirements can easily reach 6 figures. Medical school and insurance to cover all sorts of perceived malpractice easily exceeds that. It is driving doctors who have private practice and work long hours into hospital systems where they are salaried and work shifts… or retire. That doesn’t mean costs are declining, only that they are shifting. For example: http://www.kevinmd.com/blog/2014/05/pay-french-doctor.html
There are many who wonder why many Hispanics are not rushing to ACA. Here is one insight: http://www.kpbs.org/news/2010/may/19/why-americans-choose-health-care-mexico/
I suspect that, like many market-driven actions, the medical community will react to the increased regulation, massive imposed costs, legal morass, and constant scapegoating with some innovative solutions. http://watchingamerica.com/News/232437/despite-security-issues-americans-can-save-65-percent-through-medical-tourism-to-mexico/ Maybe we will begin to see hospital ships 15 miles off the coast offering treatment and recovery facilities. As long as the government continues to make life difficult for the medical industry, it will take a lot more than Medicaid to solve the problems.
Bruce Hall: You need an estimate to beat an estimate. I await your learned opinion on what is a better estimate of Rm.
Really bizarro analysis. Assumes that medicaid coverage will beat free county hospitals. Should not be worse, necessarily. But certainly those doctors choosing to accept medicaid patients will be few and far between. Hard to imagine this set up, especially with increased oversight of procedures allowed, saving money.
umes that medicaid coverage will beat free county hospitals.
As far as I know, in most counties free care by local government is nonexistent. If you have data that shows otherwise, please post it.
Guys, why are you so hard on Menzie? He is simply auditioning to be an apologist for when the mortality rate due to Obamacare sinks. He is just one of many who will be creating justification for increased mortality. They can’t admit the impact of the “death” panels and other reduced care because of “cost.” Remember, for them life is cheap and health insurance is expensive.
Ricardo an apologist for when the mortality rate due to Obamacare sinks.
A Freudian slip perhaps? Yes, I expect the mortality rate will drop. Well, eventually it’s 100%, but you know what I mean.
They can’t admit the impact of the “death” panels
Ah yes, the old death panel canard. No doubt those death panels will be staffed by Nigerian born radical gay married Marxist Muslim atheists with fake birth certificates. Did I miss any of the idiotic tropes we hear on Fox News? Oh wait, I forgot…those death panels will meet in Benghazi. And after the death panels it will be on to fight the war against Christmas.
Remember, for them life is cheap and health insurance is expensive.
I think the point of ACA is to make health insurance cheaper and available for everyone, not just rentiers on Medicare. The problem with conservatives is that only their own lives are dear; everyone else’s life is cheap. So tell us, were you one of those conservative Tea Party geezers demanding that politicians keep their government hands off Medicare?
Ricardo, I not sure what world you live where having health care leads to increased mortality! Please explain the logic behind your statement and any supporting data!
Every medical intervention carries risk and not all interventions provide greater benefits that risks.
U.S. panel recommends against PSA tests for screening … cancer in men of all ages. study finds that the … cancer blood test does more harm than good
the issue is not an occasional rio, it is does having health insurance lead to worse outcome than not having health insurance!
I wonder how many Americans died too soon, because costly, i.e. excessive, health care regulations made health care less affordable?
The ACA is creating winners and losers. However, I suspect, in general, prices will go up and/or quality will go down.
Excessive regulations have costs – in time, effort, and money, which are not limitless.
Buying health care insurance is not the same as buying health care.
We should allow the market to work, which tends to lower prices and raise both quantity and quality. So, everyone is a winner. Otherwise, there will be rationing, in one form or another,
Deregulating, while keeping appropriate regulations, will free-up enough resources to subsidize catastrophic health care or preexisting conditions, for examples, and allow a strengthening of the safety net.
Peak Trader Most of the costly and pointless regulations are there to serve the interests of those who most benefit from costly and pointless regulations. Of course, I’m talking about hospitals, drug companies and the AMA. The AMA’s whole mission in life is to restrict the supply of doctors and create rents. The marginal cost of producing most drugs is near zero. The government actually subsidizes a lot of the basic research. Big Pharma does the marketing and owns the patent rights to products that they may or may not have actually developed.
Buying health care insurance is not the same as buying health care.
True, but if you can’t obtain health insurance, then you can’t get health care. The ACA creates a market for health insurance where one did not exist before. That’s what the exchanges are.
We should allow the market to work, which tends to lower prices and raise both quantity and quality.
This is more an expression of faith than anything else. Under employer provided health insurance there is a risk of a race to the bottom due to an agency problem. Your employer sees health insurance as part of the wage bill and has no more incentive to find a plan that best suits your needs than he or she has an incentive to just give you a fat bonus just because you’re a swell guy. The employer provided model that Americans love so much is probably the worst of all possible systems. It’s worse than single payer and it’s worse than the British national health. At least under a national health system like Britain has the doctors don’t have an incentive to keep recycling patients so that they can churn out more bills to insurance companies. In Britain the doctors have a self-interest in curing you because there is no financial incentive to create repeat customers. Rich people don’t like single payer and a national health system because it doesn’t allow them the opportunity to use their dollars to jump to the head of the line so that they can get that ingrown toenail fixed ahead of the indigent heart attack victim. And the elderly don’t seem to mind a single payer system as long as it’s restricted to just them.
Otherwise, there will be rationing, in one form or another,
This is an economics blog, so it won’t come as a shock to you that there will always be rationing of some sort. When insurance companies exclude people with pre-existing conditions, that’s rationing. When only the wealthy can afford health insurance, that’s rationing.
Deregulating, while keeping appropriate regulations, will free-up enough resources to subsidize catastrophic health care or preexisting conditions, for examples, and allow a strengthening of the safety net.
This is just a pipe dream. Deregulation is a code word for allowing greater monopoly powers in health care. For example, ridiculous patent laws that benefit drug companies are significant monopoly rents that line the pockets of doctors and drug company executives. The fact is that doctors, hospitals and Big Pharma like regulations that restrict alternative choices (e.g., drugs imported from Canada). There are two ways you can subsidize health care. The first way is to overcharge subscribers that already have health insurance. Been there, done that. That’s one of the things that was driving up health insurance premiums. The second way is to tax rich people’s income and transfer it to the poor as Medicaid or Medicare. Rich folks have duped a lot of Americans into preferring the first choice. What’s wrong with Kansas?
Your suspicions about quality going down are probably wrong. Quality is being measured and monitored in the ACA programs. First time I have seen this done in any serious manner in over 40 years in medicine.
Steve
Steve, I have an HMO and a PPO dentist. The HMO dentist told me he couldn’t save a tooth. The PPO dentist saved it.
Peak Trader: QED!? So we’re at proof by anecdote, now?
Patent protection is what allows drug developers pay for the development and deployment of new drugs. No patent protection = catastrophic reduction in drug development and innovation.
Canada has cheaper prices because the government has the implicit power to bust the drug developers patents. The end result is the Canadian government is cost shifting their drug costs to US medical patients.
Might be possible to make some beneficial changes to patent law and the drug approval process but we should remember that patents have a valid purpose and have driven vast improvements in medical care and patient quality of life.
2slugbaits, the government has already done a great disservice to the American people by making health care too expensive.
Haven’t you learned anything from the public school system?
If we had a market economy in health care, it would work like any industry that’s not overregulated and/or overtaxed. There would be more output produced with fewer inputs, enormous capital creation through massive efficiencies, a faster expansion in health care, and more government tax revenue. Living standards of the masses would improve much faster.
PeakTrader,
Your comments are exactly right.
I’m glad you made the point that insurance does not equal access to healthcare. Of all the misconceptions of the Left on healthcare, this is probably the most serious. 2slugbaits illustrates the misconception in his reply to you, when, amazingly enough, he asserts that the single payer system in the UK is superior to the United States.
That just floored me. Has he never heard of the long lines? Does he not realize that people who work for big companies or who can afford it can and do buy private insurance in the UK? Does he know that people who can afford it go to Harley Street for private care. Has he ever even been to England?
Waiting times really matter. For example, if you have high stenosis in the carotid arteries and have been experiencing TIAs (transient ischemic attacks) then your risk of imminent stroke is significant. In that case, you need fast carotid imaging and quick access to carotid endarterectomy, generally within 2 weeks of the onset of TIAs. In the US, you can get that but access in the UK is limited.
I recently had an elderly family member in this situation who got immediate CTA (computerized tomography angiography) and a subsequent carotid endarterectomy (CA) in the US. If we’d been in the UK it might not have turned out so well. A Royal College of Physicians Audit showed that only one half of patients in the UK had carotid imaging (either MRI or CTA) within 12 weeks. Wait times for imaging patients at risk of stroke are rated as “significant” in the UK but “insignificant” in the US.
I’ve not seen studies on wait times for CA surgery in the US, but from what I have observed they are insignificant. However, we do know that about 30 times as many CAs per 100,000 people are performed in the US versus the UK. In the UK, only 20 percent of patients get CA within the optimal first 2 weeks and 30 percent wait more than 12 weeks.
Like I said, if you are having TIAs, you need medical attention fast to prevent a stroke. How frighteningly ironic it must be to be sitting in the UK with your universal single payer insurance, and yet you can’t get your stenosis measured quickly. And even if you could, you are unlikely to get the necessary surgery within a couple of weeks of the onset of the symptoms. Strokes aren’t pretty.
It’s possible to cite similar statistics for other problems, such as access to kidney dialysis. It’s also well known that people in the UK wait very long for access to operations that relieve pain. For example, 86% of patients in the US waited less than 3 weeks for a hip replacement. In the UK, 2% waited less than 3 weeks. On the other hand, 81% of patients in the UK waited 6 months or more for a hip replacement. In the US, 0% waited 6 months or more.
A few years ago, I was in a cab in London and I asked the driver how he liked NHS. He said, “It’s the best system in the world, isn’t it?” I asked him if he ever seriously had to use it. He said yes but it was not a great experience. When I asked what happened, he said that he was on the waiting list for gall bladder surgery and he waited so long (over a year) that it turned necrotic. I said that I recently had a family member get gall bladder surgery. He asked how long was the wait. I said 2 days. He was shocked.
I was once travelling in Wales and got sick. So I thought I’d better visit the local NHS. When I asked around, I learned that there was only one surgery in the area and it was open just one day a week. Fortunately for me, it was open the next day. (I wondered what happens to people if they get sick the day after the surgery is open.) When I went in the next day, I was horrified to see the place crammed with patients and settled in for an all day wait. Except for one thing. Since I was a foreigner, I would have to pay. So I paid 20 pounds and sat down. Guess who was the first person to be called in? Yes, indeed, me, the paying customer.
Rick Stryker Of all the misconceptions of the Left on healthcare, this is probably the most serious. 2slugbaits illustrates the misconception in his reply to you, when, amazingly enough, he asserts that the single payer system in the UK is superior to the United States.
The UK does not have a single payer system. The UK has a national health system. It is single provider. Canada has a single payer system. I don’t know how seriously anyone should take your comments if you don’t even understand the difference between single payer and single provider systems.
Has he never heard of the long lines? Does he not realize that people who work for big companies or who can afford it can and do buy private insurance in the UK? Does he know that people who can afford it go to Harley Street for private care.
I think this is the crux of the conservative argument for the bad system we have here in the US…particularly the pre-ACA US. What wealthy conservatives really want is the ability to use their wallet to cut to the front of the line. That’s what all of these arguments ultimately come down to. It’s the “ME FIRST!” argument. Long lines in the UK are a queueing problem made worse by cuts in national health. It’s an OR problem. Do you understand queueing theory? Long lines are not intrinsically part of a national health system. In fact, the usual argument from conservatives is that government run programs create excess capacity because of “empire building” incentives. Rarely do you hear someone complain that a government programs creates too little capacity. For example, that was always the Gordon Tullock argument. Governments try to do too much, not too little. Let’s do a thought experiment. Suppose the UK abolished NHS and replaced it with a US style system. What do you think would happen to observed waiting times? Actually, they would probably drop. Why? Because a lot of people who currently get healthcare through the NHS wouldn’t get any healthcare at all. If fewer people enter the system and service times are held constant, then eventually the average time in the queue will go down. The reason the UK has long waiting times is because, as in all things, big money talks and poor people walk (out the door). It wasn’t always that way with the NHS. Since we’re sharing anecdotes, long ago my wife lived in Britain for several years. But before she moved to Britain she had been fighting a chronic infection on-and-off for a long time. The US doctors kept setting up endless appointments, all kinds of tests that went nowhere and wrote out prescriptions that had no effect. But in Britain the doctors at the NHS quickly and accurately diagnosed the problem and gave her a prescription that worked. She hasn’t had that problem since. Why? Were the doctors in Britain smarter than US doctors? Unlikely. But there is one big difference and that’s the economic incentives. In the US all of the incentives lead doctors and hospitals to run patients through the system umpteen times in order to generate repeat customers and multiple insurance claims. In short, it’s a racket. In Britain the doctors have no incentive to ever want to see you again. It’s in their self-interest to solve the problem. Let me give you another example. I live near a very large university research and teaching hospital. Every woman that comes to that hospital or is seen by one of the doctors associated with that hospital (and by its nature the hospital sees lots of college aged women) always gets a pap smear test whether they need it or not. But it doesn’t end there. Since the first pap smear was so much fun, it is standard policy that a few weeks later every patient will get a vaguely alarming letter (not quite a lie, but pushing the line) that something irregular was found on the test. Nothing to worry about, but they would like to set up a second test. When this scam was ultimately exposed it turned out that it was just another case of extracting additional fees from insurance companies and increasing the experience of med students. And have you ever noticed why people who are obviously dead when the ambulance picks them up are officially kept alive (i.e., force the heart to jump and send the signal to the hospital) until they get to the emergency room? It’s because the hospital and ambulance service can charge for a live pick-up. I was shocked when a friend of mine who was an EMT explained this. Hey, the guy was obviously dead, but let’s call in the aircare helicopter so we can bill the insurance company for a few extra grand. This is an economics blog, so you really should learn to think about healthcare economics in terms of economic incentives.
Rick Stryker: You compare a system of subsidized health insurance combined with personal mandates operating with privately owned suppliers, originally conceived by the Heritage Foundation, to a government operated system in the UK, rather than more similar systems operating in France and Switzerland. Hmm. I look forward to more anecdotes from you.
Should check the assumptions in the study being discussed. It says
The Oregon study concluded
The Oregon study showed that when people were given access to medicaid there were no improvements in measurable indicators of health.
Those results question the simplistic assumption that access to medicaid improves health and reduces mortality.
The Oregon study was underpowered. The more recent Massachusetts study had enough people to generate useful data. It also had some problems with disparities in the sizes being compared, but was large enough to find what you were looking for.
Steve
Duracomm: It is usually helpful to provide the links to relevant articles being quoted so others can assess (isn’t that the point of the internet world and blogs). Since you have not done so, let me provide the caveats the authors provide in what I believe is the source article:
I think you might find it useful to consider the estimates regarding mental health (included in the analysis conducted by Dickman et al.), as well as catastrophic health costs and financial impact.
Menzie,
If readers followed the link you kindly provided to the opting out study they would find the Oregon study I cited is the the first link (click on the “recent studies” text in the first sentence of the second paragraph) in the opting out study.
The text you cite on the limitations of the Oregon study raises this interesting point
This brings up the possibility that expanding medicaid will cause increased wait times due to increased demand for limited medicaid provider resources. The result of this would be overall worse health outcomes because the sick would have delayed access to medicaid services.
Not a guaranteed negative outcome but certainly a plausible one.
Which reinforces my original point that the assumption that access to medicaid improves health and reduces mortality is simplistic and needs to be carefully considered.
Duracomm This brings up the possibility that expanding medicaid will cause increased wait times due to increased demand for limited medicaid provider resources. The result of this would be overall worse health outcomes because the sick would have delayed access to medicaid services.
Huh? Did you think that through? I believe you meant to say that those who already have insurance might suffer a worse outcome under Medicaid expansion if the system’s capacity is strained. Of course, it’s exactly the opposite for those that didn’t have any insurance before ACA and Medicaid expansion. The odds will improve for those people. Again, you are really making the same argument that Rick Stryker was making. In your world it’s a crime against humanity if healthcare for a rich person suffers and Grandpa Bigbucks has to wait for his elective surgery. But if the less fortunate and poor suffer adverse outcomes because they don’t have any insurance…well, life’s unfair and they will just have to accept their sorry lot. Those people simply don’t count.
Have you noticed a theme here? It sounds a lot like Mitt Romney’s 47% comment. The “good people” work hard and contribute to the economy. They deserve first class medical treatment. Obviously they should always be at the head of the line. Hey, first class airline tickets mean you get to board the plane first (I guess so they can get drunk faster), so it should be the same with healthcare. But what about health insurance for the poor? You know…”those people.” Well, I guess it’s okay as long as they’re having access to healthcare doesn’t inconvenience “the good people” or mean Grandpa Bigbucks has to wait like the rest of us mere mortals.
The map itself is revealing. There are some exceptions, but for the most part it’s pretty easy to tell which governorships and legislatures are controlled by the “stupid party.” On the other hand, it looks like Jefferson Davis’ descendants might want to kick Arkansas out of the Old Confederacy.
2slugbaits,
1. You are mixing private insurance and medicaid confusing two different issues.
2. If medicaid expansion increases the number of healthy people using limited medicaid resources the ability of sick people to access medicaid resources is reduced. Not a guaranteed outcome but a plausible one that is reasonable to assess.
3. The class warfare rant was entertaining but uninformative.
Rick Stryker: “It’s possible to cite similar statistics for other problems, such as access to kidney dialysis. It’s also well known that people in the UK wait very long for access to operations that relieve pain. For example, 86% of patients in the US waited less than 3 weeks for a hip replacement.”
It’s always amusing when conservatives cite hip replacements in their attacks on government health care given that three-quarters of all U.S. hip replacements are paid for by that socialist menace, Medicare.
Likewise for kidney dialysis. For 40 years, through a special rule, dialysis is the only medical condition for which Medicare has provided coverage for everyone regardless of age.
Given that Stryker cites these as examples of what is right about U.S. healthcare, it seems that he is making a good case for Medicare for all.
Menzie,
I was reacting to 2slugs’ assertion that the UK health system is better than the US. That’s why I compared to the UK rather than France or Switzerland. Moreover, I was not drawing general conclusions from anecdotes, as you seem to be suggesting. Rather, I cited statistics and then buttressed them with some personal anecdotes.
You are repeating the false claim that the ACA was invented by the Heritage Foundation and Romney. I can only assume that you have been influenced by Krugman’s ontological argument for the existence of Obamacare. According to Krugman’s argument, Obamacare exists as it does because it must exist as it does in order to solve the health care policy problem. Therefore, if the Heritage Foundation and Romney invented a solution, it must be the ACA.
That’s nonsense of course and a re-write of history. Romney and the Heritage Foundation did not invent Obamacare and do not support it. As Romney explained during the campaign, Romneycare was designed for the specific circumstances in Massachusetts and is not generalizable to Obamacare for everyone. Romney’s plan had very important differences from Obamacare.
Rick Stryker: I didn’t say all ACA was thought up at Heritage. Individual mandates in a system of insurance with subsidies were — read it at this Heritage document, pp. 51-52. This is a chapter written by the Director of Domestic Policy at Heritage, in a Heritage document, on a Heritage website, so…
Menzie,
Well, that’s the document that Krugman pointed to to claim that conservatives used to support the essential ideas of Obamacare. I think the truth is a lot more complicated. Thought you might be interested in how support of the mandate evolved among conservatives.
When Heritage wrote that 25 years ago, (Stuart Butler in particular) the context was very much the Emergency Medical Treatment and Active Labor Act (EMTALA), passed in 1986, that required hospitals to provide emergency treatment without regard to ability to pay. Given that emergency treatment was now funded by taxpayers, some conservatives believed that the unfunded mandate should just be made explicit and fall directly on people by requiring them to purchase some sort of insurance rather than have people pay indirectly in higher premium costs and/or taxes. Many conservatives in the early 1990s took up the mantle of the idea of a mandate, notably Milton Friedman and Newt Gingrich.
At the same time, many other conservatives strongly opposed the idea. Peter Ferrara, who also authored a chapter of the 1989 Heritage document, quit Heritage over the mandate. He subsequently organized conservatives to oppose the mandate. Ferrara’s concern was that once a mandate is in place, the government would use it to extend the insurance requirements necessary to satisfy the mandate so that people will end up being forced to buy very expensive and comprehensive insurance rather than the catastrophic insurance that many supporters of the mandate originally intended.
For example, Romney’s original conception was for a very soft mandate, very much motivated by the desire to clarify and focus the costs of the EMTALA directly on people rather than to hide the costs under an unfunded mandate. Under the original Romneycare, people would be required to either purchase catastrophic insurance that would cover the cost of emergency care or post a 10,000 bond to cover that care. If people did neither, then they would lose their personal tax exemption until the cumulative tax increase equalled the 10,000 dollar bond.
Romney felt that he could impose that requirement since he expected deregulated, cheap catastrophic insurance would be available through the connector. The connector, which was in fact a Heritage idea, was designed to be an exchange in which insurance would be deregulated and all manner of insurance policies could be sold. The connector was supposed to unite the individual and small business markets. In the original idea, businesses could send employees to the connector to buy insurance. People could take a contribution from their employer to purchase insurance before tax and for the first time could take their spouse’s employer’s contribution to the connector as well. If someone has two jobs, he could use a contribution from both employers. And the connector would allow insurance to be disconnected from a job and hence portable. In other words, insurance could be defined contribution rather than defined benefit.
As in the 1990s, this was controversial among conservatives. Conservatives understood that Romney was working within the particular constraints of Massachusetts, but many thought that the mandate and connector would not work out as Romney intended. And indeed, these critics were right. The democratic legislature added for example an employer mandate, which Romney vetoed, but which was overidden. Moreover, the new Deval Patrick Administration changed the original concept so that it ended up looking very much like the ACA today. Insurance policies became more regulated on the connector, with bronze, silver, and gold policies defined. The mandate morphed into a penalty that was based on income on a sliding scale and tied to the lowest cost Bronze plan provided on the connector. Ultimately, the ACA would be modeled on the Deval Patrick Adiminstration’s reinterpretation of Romneycare.
As a result of this experience, conservatives who had supported the mandate as a tactical matter pretty much joined the side of those who warned that the mandate would be used to create even more regulation of insurance. By the time of the ACA, almost all conservatives were opposed to the mandate, including the Heritage Foundation, which filed this amicus brief against the mandate. Romney himself did not support the mandate and neither did Stuart Butler. ACA became purely a Democratic policy and no Republicans supported it.
stryker,
the republican’s quit supporting romneycare when it was renamed obamacare after our first democratic black president. the essence of the programs are the same. you are trying to use technicalities to differentiate between the two and distance past support for the same “nameless” program. the right argues the programs are totally different, because our program used “The” in the title, and their program used “the” in the title. totally different! its the kind of argument you hear from students caught plagiarizing!
Joseph,
That’s certainly peculiar logic. The fact the Medicare within the context of a multi-payer private system delivers shorter waiting times than the single-payer socialized medical system in the UK does not imply that therefore Medicare should be expanded. It just implies that the UK would get better results moving towards the US system, at least as far as waiting times are concerned.
You also missed my point on dialysis. My comment was about waiting times and so of course that’s what I meant by access to dialysis. Hemodialysis requires repeated access to the intervascular system, access that is robust over long periods of time. The gold standard for access is arteriovenous fistula. To get that, a patient needs timely access to a dialysis surgeon. An arteriovenous fistula is constructed by connecting a vein to an artery. After the fistula is created, it might take anywhere from weeks to months for the fistula to develop to the point at which it can be used for dialysis. In the meantime, the patient will have to use a less effective method, such as a catheter.
Relative to catheters, fistulas have lower rates of infection, better blood flow, reduced clotting, and lower maintenance costs. Thus, waiting time for fistula surgery is important for the health of a dialysis patient. So what are the facts on waiting times? Typical waiting times from referral to surgery is 62 days in Canada, 30 days in Europe, and 16 days in the USA.
Your comment about dialysis being available to everyone under Medicare is misleading. You can qualify for Medicare if you have end stage renal disease and either 1) you’ve worked the required time under social security, the Railroad Retirement Board, or as a government employee; 2) you are collecting or eligible for social security or Railroad Retirement benefits; or 3) you are the spouse of dependent child of someone satisfying 1) or 2). After you enroll in Medicare (if you qualify), benefits would in general start in the fourth month of dialysis (there are ways to avoid that), subject to the deductible and 20% co-pay. Importantly, Medicare does not cover the arteriovenous fistula surgery.
2slugbaits,
As usual, I’m not sure what to do with your comment, since you are all over the map.
You start with semantics–the distinction between single payer and single provider. But who cares? How is this relevant to the argument? Besides, your distinction isn’t even right. See for example the wikipedia article Single Payer Health Care that notes that both Canada and the UK are examples of single payer. But it wouldn’t matter if your distinction were right.
You then move right on cue into the standard Left wing technique of attacking motives. Your most amusing claim is that US doctors don’t have an incentive to cure their patients, since by not curing them they can keep charging them. But you assert that doctors in the UK want to cure you, since they don’t get to charge you twice and don’t want to see you again.
Do you honestly believe this? I wonder what any US doctors who might be reading this blog think of your argument.
Stryker, you crack me up. When two shining examples of U.S. health care that you pointed out are revealed to be primarily due to Medicare, you twist yourself in knots to back out of it. Cognitive dissonance must be one hell of a drug.
More government micromanagement in health care will cause more undesirable effects.
I think, people are in for a rude awakening. Of course, politicians will shift blame.
For example, according to “Comparing the U.S. and Canadian Health Care Systems – NBER:”
“Finally, the authors examine whether Canada has a more equitable distribution of health outcomes, as might be expected in a single-payer system with universal coverage. To do so, they estimate the correlation across individuals in their personal income and personal health status and compare this for the two countries. Surprisingly, they find that the health-income gradient is actually more prominent in Canada than in the U.S.”
http://www.nber.org/bah/fall07/w13429.html
Isn’t it possible that ALL medical payment systems are severely flawed in one way or other?
Just as democracy is merely the least bad system of government. I’ve used the UK National Health – a mess in practice but cheap in GDP terms; the French system – great if you are eligible and speak French; the US Army as an enlisted man – like an mega-enema; and now Medicare – good if you can work the system.
As to health outcomes, why would they improve much in the US regardless of the system?
The bottom 20% or so of US society who are uninsured include many/most of our high school drop-outs and the morbidly obese and the smokers – these factors overlap and are inevitably going to produce poor health outcomes. Keeping such folks alive longer by providing, for example, free diabetes amputations may be desirable for reasons that aren’t medical – like the political needs of liberals. Or is such care a cruel joke on the sufferers and an unnecessary cost for society? These are political questions, not medical ones.
Personally – being a little closer to the end than most posters on this website, I’d prefer a cheap and cheerful and dignified exit – which US medicine doesn’t offer.
PeakTradeer, that paper is one fine piece of work. Why am I not surprised that it comes from an AEI staffer.
This is what the paper shows:
If you don’t count all of the underweight babies in the U.S. — infant mortality rates are almost the same!
If you don’t count poor minorities in the U.S. — medical outcomes are almost the same!
If you don’t count the uninsured in the U.S. who wait forever — wait times are almost the same!
But the kicker is that even after all of the cherry picking, they find that the U.S. is slightly better in some metrics and the Canadians are slightly better in others. And the bottom line is that the Canadians spend just a little more than half what the U.S. does per person while covering 100% of their citizens. The U.S. really does have the worst health system in the world. No better outcome at twice the price!
Do the Canadians – or Finns or Japanese – have a huge and growing black and Hispanic underclass that the rest of us never noticed? Is it unbearably racist to take that into account?
The UK has had single payer since the 1940s but inner Glasgow has third world mortality numbers – for whites. GIGO applies to health just as with everything else.
Joseph, you’re making implications, e.g. all minorities are poor, and twisting the study, e.g. declaring the uninsured wait forever. For example, the study states: “While the incidence of unmet needs is slightly lower in Canada (11 percent, vs. 14 percent in the U.S.), it is interesting to note that waiting time is cited as the reason by over half of Canadians who report unmet needs. By contrast, cost is cited as the reason by over half of Americans.”
Less than 3% of Canada’s population is black and less than 2% is Hispanic. The data show blacks have a lower life expectancy and most immigrants to the U.S. come from dirt poor countries (a small proportion of them are highly skilled or educated, which adds to income inequality).
A rigorous study, comparing health care systems, compares apples to apples, , e.g. the NBER study.
When you say the U.S. spends more on health care per capita than other countries, you seem to ignore the fact that it includes more research and development, more and better capital equipment, more and better clinics and hospitals, higher quality treatments, highly specialized doctors, etc..
The U.S. is #1 in the world in both labor (e.g. doctors, nurses, specialists, etc.) and in capital (e.g. hospitals, equipment, technology, etc.). I’m sure, the U.S. is also #1 in the world in research and development, and in new therapies and drugs, which not only benefit the U.S., they benefit the rest of the world.
Joseph,
I did not try to back out of anything. I merely pointed out that your logic doesn’t make sense and that your Medicare factoid was misleading.
Just to restate: If I had compared medicare to a free market system and medicare had longer wait times, then you’d have some basis to claim that we should therefore expand medicare. But I didn’t do that. I compared the mixed US system to NHS in the UK. The US has clearly lower wait times for important procedures. From that, you simply can’t argue that we should therefore expand medicare.
In my reply, I also compared wait times between the Canada and the US. The Canadian system is already similar to a vastly expanded medicare. And yet wait times are much longer for arteriovenous fistula surgery in Canada vs. the US. How does that square with your claim that we should therefore expand Medicare?
I’m not surprised that you respond with mockery and accusations of cognitive dissonance. Your logic is clearly wrong and you need to distract attention from that.
Sorry, just saw a typo: my comment above should read:
If I had compared medicare to a free market system and the free market system had longer wait times, then you’d have some basis to claim that we should therefore expand medicare.
You might compare Medicare, free market system and those who have no insurance
Also, when controlling for factors outside health care systems, the U.S. has the best health outcomes in the world, including the longest life expectancy.
Beyond Those Health Care Numbers
“The difference in health outcomes has more to do with broader social forces.
Americans are more likely than Canadians to die by accident or by homicide. For men in their 20s, mortality rates are more than 50 percent higher in the United States than in Canada…accidents and homicides account for most of that gap.
Americans are also more likely to be obese, leading to heart disease and other medical problems. Among Americans, 31 percent of men and 33 percent of women have a body mass index of at least 30, a definition of obesity, versus 17 percent of men and 19 percent of women in Canada. Japan, which has the longest life expectancy among major nations, has obesity rates of about 3 percent.
The health system in the United States gives low birth-weight babies slightly better survival chances than does Canada’s, but the more pronounced difference is the frequency of these cases. In the United States, 7.5 percent of babies are born weighing less than 2,500 grams (about 5.5 pounds), compared with 5.7 percent in Canada. In both nations, these infants have more than 10 times the mortality rate of larger babies.
Research by the Harvard economists David Cutler, Ed Glaeser and Jesse Shapiro concludes that America’s growing obesity problem is largely attributable to our economy’s ability to supply high-calorie foods cheaply. Lower prices increase food consumption, sometimes beyond the point of optimal health.
Science has consistently found new ways to extend and improve our lives. Wonderful as they are, they do not come cheap.”
http://www.nytimes.com/2007/11/04/business/04view.html?_r=0
Slug,
You are right. I did make a mistake discussing mortality.
Robert Hirley,
You apparently know nothing about the UK National Institute of Health.
Ricardo: Earth to Ricardo. Robert Hirley might not know anything about the UK National Institute of Health because it doesn’t exist. There is a National Institutes of Health in the United States, and there’s a UK National Institute of Health and Care Excellence. But there’s no organization with the name you referenced. Could you have meant the UK National Health Service, which delivers health care?
ricardo
“They can’t admit the impact of the “death” panels and other reduced care because of “cost.” Remember, for them life is cheap and health insurance is expensive.”
i love it. now that ricardo is collecting medicare, we should not control costs on this subsidized social medical program in which he is enrolled. don’t you dare touch his entitlements! hypocrite! and you wonder why nobody takes you seriously?