From “Estimation of Excess Deaths Associated With the COVID-19 Pandemicin the United States, March to May 2020,” JAMA, today:
Across the United States, there were 95 235 reported deaths officially attributed to COVID-19 from March 1 to May 30, 2020. In comparison, there were an estimated 122 300 (95% prediction interval, 116 800-127 000) excess deaths during the same period (Table). The deaths officially attributed to COVID-19 accounted for 78% of the excess all-cause deaths, leaving 22% unattributed to COVID-19. The proportion of excess deaths that were attributed to COVID-19 varied between states and increased over time (Table and Figure 1).
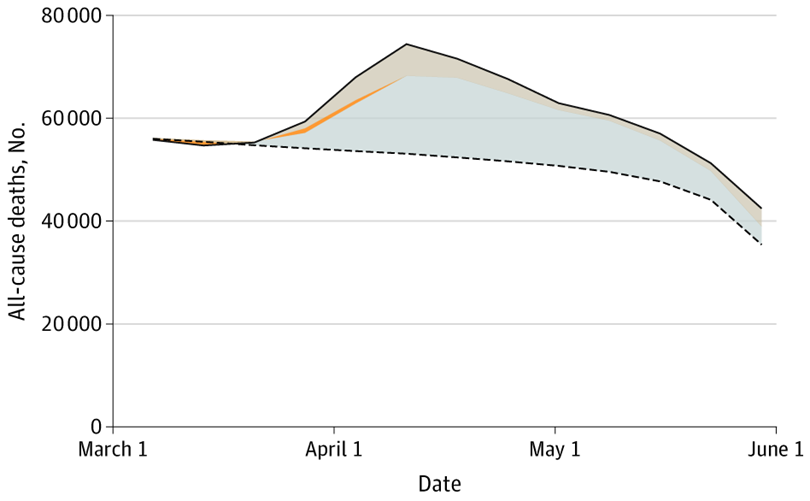
Figure 1: Excess Deaths in the United States From March 1 Through May 30, 2020. The observed number of deaths is indicated by the solid line, and the expected number of deaths, adjusting for seasonality, influenza epidemics, and reporting delays, is indicated by the dashed line. The area between these 2 lines represents the total number of excess deaths: blue-gray (bottom), deaths recorded as due to COVID-19; orange (narrow middle section), additional pneumonia and influenza excess deaths not coded as due to COVID-19; and beige (top), deaths that were not attributed to COVID-19, pneumonia, or influenza.
This implies a point estimate for undercount of Covid-19 fatalities by 27,000 for the March-May period.
(This approach is not persuasive if you thought the excess deaths were primarily people who were going to die in the very near future; for examples, see the excess fatalities debate for Puerto Rico/Hurricane Maria.)
In the JAMA article, I didn’t notice any adjustment for March-May driving fatalities being lower than expected (based on the non-pandemic past). Assuming no such adjustment, the undercount is probably higher than what Weinberger, et al. (2020) report.
Not in March, interestingly.
https://ohsonline.com/articles/2020/05/22/motor-vehicle-fatality-rates-up-14-percent-in-march-despite-covid19.aspx
you are trying to compare changes in rates to changes in magnitude, steven.
@ PrincetonKopits
Is there any truth to the rumor you were going to do some long-form journalism for “National Review” provisionally titled “Excess Brown People Deaths, Excess Low Income Elderly Deaths, Why Neither Really Matter” ??
If you did indeed come up with that title Kopits, I gotta hand it to yeh, it is a “click-bait” worthy title. I bet Ed Henry (girls out there reading this, never trust a man with two first names) would invite you on his new podcast to promote that.
How bad is Wikipedia? Under its current description of the Hurricane Maria death controversy, there is this tidbit:
“Steven Kopits of Princeton Policy Advisers conveyed that if the study were to be believed, approximately 3,000 bodies would be missing whereas only 45 people were reported missing by the end of December 2017.”
Wikipedia allows any fool to edit this accounts. I bet Stevie pooh slipped this into the account so he could get another call from Fox and Friends.
@ pgl
Nice catch, I would say that is a very astute theory you have there. I think I’d take your same side of the bet there if that was offered as a wager in Vegas. Or someone Kopits put up to it, for certain. I do think Wiki does more good than bad. But little inputs like that will leave you wondering if there’s a better way of administering the Wikipedia site.
The good news is anyone who is actually literate is probably going to “catch that” just like you did. But when people are busy that might be the type thing glanced at and missed.
If anyone is interested in “anecdotal evidence”, I am here to tell you in the last month or so, even up to today, the amount of “bad driving” or “overly risky driving” which could result in fatalities has risen dramatically in the state that I reside in. I would be literally shocked and awe-struck if the amount of severe accidents as a ratio of cars commuting on the roads hasn’t risen dramatically. My “Joe Six-Pack Theory” on this, is that drivers have figured out they are much less apt to be pulled over for a citation due to police fears of contracting the virus with interactions with the general public on traffic stops,
Even redencks “pick up” on these things (a break in usual police habits) very fast.
I read the paper this morning. While the extrapolation is OK, we still don’t have any good handle on the number of viral infections. The big number everyone wants to know is the case fatality rate (CFR). We still don’t know what the true level of infection in the US is. Even when that data has been published it involves an extrapolation. The only way to get at all this is to do much more testing (duh!!!) and for the deaths, tissue samples really need to be analyzed for the presence of virus. I still have not changed my thinking that the CFR is in the range of 0.3-0.6% which is much higher than typical seasonal influenza.
” The big number everyone wants to know is the case fatality rate (CFR).”
No, the big number is the “infection fatality rate” (IFR). 🙂
I still have not changed my thinking that the CFR is in the range of 0.3-0.6% which is much higher than typical seasonal influenza.
The IFR is indeed in the 0.5% range: the age corrected IFR on the “Diamond Princess” is around 0.6%, the preliminary antibody tests in Austria and Germany point to a value in the 0.3% – 0.8% range. All this of course with sufficient number of ICU beds.
For Germany we have a mortality of intubated patients of 25-30%. However,an overwhelmed hospital system would have 3-4 times higher IFR, 1-2%, that is a lot.
I would think fatality rates by age & risk group would be more useful than a global average. The global average CFR might be in the 0.3%-0.6% range, but I am more concerned about the conditional CFR. It’s the conditional risk that governs my choices, not the unconditional risk. Also, in terms of the economics, we put too much emphasis on the number of deaths. We should also recognize that even a favorable outcome incurs significant economic costs. An infected person is out of the workplace for 3-4 weeks assuming all goes well. Hospital beds and emergency rooms filled with COVID cases are hospital beds not filled with cardiac or stroke patients. Increased medical costs add to GDP, but in the same way that capital depreciation adds to GDP. And that’s perverse. What we should really focus on is NDP that recognizes health maintenance as the equivalent of a capital depreciation cost. Welfare matters.
Remember, according to Steven Kopits, there are no “excess” deaths. There are only “slightly premature” deaths of people destined to die anyway. And because of these premature deaths we will enjoy a future reduction in deaths because all the weak ones were killed off.
It would be interesting to revisit mortality in PR two years on.
@ PrincetonKopits
I wouldn’t if I were you. You revisiting Puerto Rico excess deaths is like Reinhart and Rogoff revisiting Excel spreadsheets. And really, that’s an insult to Reinhart and Rogoff.
Relating Maria to this COVID issue:
https://www.arkansasonline.com/news/2020/jun/27/the-hidden-deaths-of-the-covid-pandemic/
Since Princeton Stevie pooh asked – this article noted the official for Maria 2 was 2975 while a Harvard analysis suggested it was 4600.
A wee bit more than Stevie pooh’s 64. Of course Trump told us only one American would die from COVID.
CDC reported weekly deaths as of 7/2. https://scontent-ort2-1.xx.fbcdn.net/v/t1.0-9/106501024_783139159169965_883907068016827749_o.jpg?_nc_cat=109&_nc_sid=ca434c&_nc_ohc=ILgoCa2xuo4AX9mlb3n&_nc_ht=scontent-ort2-1.xx&oh=dd60a207644f708bd9d29aca73d54d64&oe=5F2362D2
Regarding excess deaths, you may be interested in this analysis of the Ferguson et al. study. https://www.nicholaslewis.org/wp-content/uploads/2020/03/COVID-19-Diamond-Princess-based-analysis_Lewis_27Mar20a.pdf
I don’t know if the JAMA and Ferguson projections are consistent.
Bruce Hall: CDC website makes explicit reference to *not* taking at face value the most recent weeks’ worth of data, because they are preliminary. Those data are marked as such (i.e., column Q) in the original spreadsheet CDC provides, so it makes sense to exclude most recent weeks. In my post on excess deaths, I excluded the most recent month.
I think that’s what the note on the chart indicates. It will be interesting to follow the changes over the next few weeks to see the changes. If the headlines about cases are an indication, then the red line should reverse dramatically.
“It will be interesting to follow the changes over the next few weeks to see the changes.”
And if the number of deaths climb, the liar Bruce Hall will just disappear. You always do.
“I think that’s what the note on the chart indicates.”
And you failed to mention this in your comment. Just like you failed to mention the 1st time you used this 2nd hand source rather than linking to the CDC website. Which is why everyone here knows you love to misrepresent just about everything.
pgl,
sorry that I overestimated you ability to read the chart. Do you have the same issue when Menzie posts a chart based on data from his sources? The image clearly shows the source of the data, but perhaps you require a larger font and bolding of the text.
“Bruce Hall
July 2, 2020 at 3:25 pm
pgl, sorry that I overestimated you ability to read the chart. ”
Bruce Hall is a sad little pathetic boy. I can read charts. My point is that you love to misrepresent everything. I wish for once you would admit the fact that you are a serial liar. But no – when someone calls you on your dishonesty, you fire off some stupid insult like that. An insult without foundation.
Wake me when you are ready to have an honest discussion. Snicker.
pgl,
your lack of thoroughness is my dishonesty? I’ll have to give you another asterisk for that one.
Bruce Hall: No, your graph merely indicates that data are subject to revision, but not that the more recent data are preliminary, and hence more subject to revision. The graph you linked to had one vertical line, which did *not* define the preliminary data.
I bet Bruce was fully aware of this. No – Bruce is not as stupid as he comes across. He is just being paid to lie for Team Trump.
Menzie,
Almost all of the data appear “preliminary” if you look beyond the chart to the data. If I had posted all of the footnotes from the CDC source report (which was shown on the graphic). I would have been accused of insulting everyone’s intelligence.
Meanwhile:
https://reason.com/2020/07/01/covid-19-herd-immunity-is-much-closer-than-antibody-tests-suggest-say-2-new-studies/
I know, I know… pgl won’t like the source of the article and will ignore the study itself.
Bruce Hall: Well, when I used the data, I noted in the text that data were preliminary, and I investigated how much the data was revised in releases week-by-week so I could determine when it made sense to truncate the data given likely revisions. So…I’ll just say one has more credibility when (1) original source data is used, and (2) one treats the data carefully…(both are what I tell my students).
This is the 2nd time Bruce peddled this single statistic second hand sourced link:
https://scontent-ort2-1.xx.fbcdn.net/v/t1.0-9/106501024_783139159169965_883907068016827749_o.jpg?_nc_cat=109&_nc_sid=ca434c&_nc_ohc=ILgoCa2xuo4AX9mlb3n&_nc_ht=scontent-ort2-1.xx&oh=dd60a207644f708bd9d29aca73d54d64&oe=5F2362D2
The first time he peddled this – I provided him links to the original CDC source. It seems Bruce choose not to go to the actual CDC data. Same old Bruce – peddling second hand intellectual garbage.
pgl,
the CDC provides weekly updates, not weekly comparisons of their report. The chart simply takes the data from the CDC report and shows the changes. I’ll continue to provide the comparisons regardless of your objections which are sophomoric.
https://data.cdc.gov/NCHS/Provisional-COVID-19-Death-Counts-by-Week-Ending-D/r8kw-7aab
Stop the presses. Brucie finally decided to link to an original and reliable source. I’m sorry Brucie but you will be fired by the close of week by Team Trump. So it seems you will have to take that job in the meat packing plant. Hint – wear a mask.
, does “finally” mean you finally looked at the link I’ve posted/referenced several times?
You are peddling more intellectual garbage from Nic Lewis? Hey – John Lott calls himself a statistician. Why not find some of his misleading work too?
pgl, you appear desperate in your attempt to be a critic of all sources not pgl
Simply state your specific issues with the analysis rather than slither in the gutter of ad hominem remarks. This is, after all, a data-driven blog. Try being a data-driven critic.
And don’t ask for all of the footnotes. Go to the provided sources and examine them yourself.
Nic Lewis’s intellectual garbage has already been shredded by others. Come on Brucie – do pay attention.
Now, p, we know that disagreeing is not the same as “shredding”. One needs more than scoffing to dispute an assertion.
“One needs more than scoffing to dispute an assertion.”
If you go back and actually READ the comments to that first Nic Lewis thing you posted, you would see at least one well informed person shredding the crap out of what he wrote. Oh wait – you generally don’t even bother to get past the headline of most of the stuff you linked to. Asking YOU to read is clearly asking for too much. So troll on dude!
pgl, the comments ranged from pgl to supportive.
It seems as if the analysis depends on which way the coin lands.
• https://www.msn.com/en-ca/health/medical/people-are-dying-of-illnesses-other-than-covid-19-because-they-wait-too-long-to-seek-help/ar-BB12K9wx
• https://www.nytimes.com/2020/06/09/opinion/coronavirus-hospitals-deaths.html
• https://www.fox43.com/article/news/local/cardiac-arrest-cases-rise-during-covid19-pandemic/521-83c0c6d0-7212-4d86-aa70-9387d750939f
Bruce Hall So what point are you trying to maker with those links? It seems to me that if someone dies from a heart attack because they wait too long to go to the hospital or can’t get an EMT to show up because of COVID-19, then that ought to count as a COVID-19 death just as much as if the person died directly from COVID-19.
‘So what point are you trying to maker with those links?’
Brucie never has a point. He is just following orders from Kayleigh McEnany.
this argument by bruce is consistent with the illogical argument he has made that shutting down the economy and eliminating elective procedures caused more deaths because people with elective procedures could not get to the hospital. first, these were elective procedures and not emergency procedures. and second, if you did not shut things down at first, you would have flooded the hospital with covid patients. and this is exactly what we are seeing today. bruce hall is making an illogical and inconsistent argument, and he is actually serious about this argument. makes you wonder how good of an analyst he was before he was terminated.
baffling,
The links were not about elective procedures specifically. They were about the reluctance of people to go to the hospital when symptoms indicated they should. This included people with serious heart conditions and cancer. I’ll leave up to you whether you actually want to read them or not. The point is that some people may be dying unnecessarily due to their fear of the well-hyped Covid-19 virus as pointed out by EMTs in the last article. Yes, it’s anecdotal, so we got that out of the way.
By the way, let’s put to rest the arguments about case counts and death counts. Let’s accept they are estimates made by the government and we have no better sources at this time. Or do you wish to object to estimates? Then let’s do away with most economic data while we’re at it. We’ll just let pgl tell us everything.
By the way all of you medical experts: https://www.detroitnews.com/story/news/local/michigan/2020/07/02/michigan-henry-ford-health-study-finds-hydroxychloroquine-lowers-covid-19-death-rate/5365090002/ I know that pgl will want to see the study details and will object to this link as second or third hand.
Bruce Hall No surprise that so many of your links are to the hard right Detroit News. But I digress. First, did you notice that the study outcomes were both within the global mortality rate range for hospitalized COVID cases? And did you notice that hydroxychloroquine was not the only treatment difference but was only one element of a suite treatments including enhanced monitoring of cardiac issues for patients with hydroxychloroquine. So it’s quite a leap to attribute the favorable outcomes to hydroxychloroquine alone. And if you had followed the links you would have learned that those patients receiving hydroxychloroquine were not randomly selected candidates but those not getting the hydroxychloroquine treatment were randomly selected. Is that your idea of good study design? And did you catch that part whether other hospital groups in the Detroit/Ann Arbor area disagreed with the Henry Ford group’s conclusion? The benefits of hydroxychloroquine remain unproven. Some studies suggests benefits, other studies fail to find benefits. That’s how most studies go until we get a lot more studies until eventually the weight of the evidence falls on one side or the other. As of right now you cannot claim that hydroxychloroquine has a proven benefit although you can say that it has a proven risk.
So let’s review some of your claims surrounding the COVID-19 virus:
(1) You assured us that it was no worse than the flu. You were wrong.
(2) You were confident that it was seasonal and would go away with warmer temperatures. You were wrong.
(3) You claimed that hydroxychloroquine was an effective treatment for COVID-19. At best your claim is unproven. At worst it’s outright wrong and dangerous.
A few days ago you indicated that you don’t wear a mask. Still feel that way now that the hosts at Fox News have had their “come to Jesus” moment and are now urging everyone to wear a mask?
“The point is that some people may be dying unnecessarily due to their fear of the well-hyped Covid-19 virus as pointed out by EMTs in the last article.”
as i pointed out before, for those unable to read, then you endorse an approach that minimizes the severity of covid. and the result is a hospital overrun by covid patients. so those “heart attacks” still are not treated. see houston as a case study today. the proper approach is a strong commitment to social distancing, face masks, and controlled economic reopening that limits the circulation of the virus in a community, frees up hospital resources, and permits people to seek needed medical care without the threat of catching the virus. and this is the path forward until we reach either a vaccine or effective large scale therapeutic. it is not rocket science bruce, although it may appear as such to you.
2slug,
Covid-19 mortality is ?. If you take the latest CDC comments regarding all infections including asymptomatic (not just reported cases … https://www.nbcnews.com/health/health-news/cdc-says-covid-19-cases-u-s-may-be-10-n1232134 … remember that link I provided previously), the mortality rate is roughly 0.5% in the U.S. with 43% of the “official” deaths occurring in concentration camp nursing homes (NYT – thank you Govs. Cuomo and Whitmer for your policies). This brings it closely in line with the 1968 flu which also killed mainly older people.
BTW, my 69-year old brother-in-law just got infected with Covid-19. He went to the ER, got some treatments and now says he feels quite a bit better. Yeah, that’s anecdotal. But I digress.
With regard to the study at Henry Ford Health Systems (one of the largest in Michigan), what does the reporting source have to do with the validity of the report? Did they report it incorrectly? Did they fail to provide counter-arguments? It didn’t align with your political agenda? It’s just a study with some positive results. U of M hospitals don’t use it. Others do. I’m sure protocols still vary. Kind of like economists who look at the same data and pronounce diametrically opposed opinions.
I’ve notice a lot of you like to express opinions, but don’t really want to discuss data. You seem content to scoff at the work of others without bringing anything to the table yourselves. So why don’t your provide an analysis of Dr. Lewis’ article in terms of what he wrote, not snide comments that some others might have made. You might have guess by now that I don’t give a lot of weight to snide comments, but I don’t mind addressing them.
Oh, 2slug et al. don’t like “conservative” sources; e.g., The Detroit News. How about The Hill? That provides a variety of perspectives.
https://thehill.com/policy/healthcare/505801-study-ties-hydroxychloroquine-use-to-lower-covid-19-death-rate
Oh, my. the HFHS results were different because they used a different protocol and different dosing than the other studies. Well, that’s cheating… right 2slug? Obviously a right-wing conspiracy.
Bruce Hall what does the reporting source have to do with the validity of the report? Did they report it incorrectly?
The problem with the Detroit News is that they didn’t tell the whole story. Their version was very misleading. It didn’t include a lot of the cautionary notes that even the authors of the study pointed out. It was an unbalanced piece of reporting.
Did they fail to provide counter-arguments?
Yes, they did fail to provide counter-arguments. They failed to point out that the outcomes in the test were within the range of global outcomes. They failed to report that the test subjects receiving hydroxychloroquine were not randomly selected. They failed to point out that the two groups of patients received very different treatments that differed by more than just hydroxychloroquine.
don’t really want to discuss data
I do discuss the data. What do you think I just did? You’re the one who will not or cannot discuss data. Instead, you just post links without even understanding what your sources are saying. Remember, you’re the one who struggled with logarithms.
“The findings have been highly analyzed and peer-reviewed,” Marcus Zervos, co-author of the study and division head of Infectious Disease for Henry Ford Health System, said in a statement.
Peer-reviewed? Really? That’s a term that a lot of people (particularly on the right) have been abusing. I suspect that the study is more likely a working paper that was passed around some friends for quick comment.
the HFHS results were different because they used a different protocol and different dosing than the other studies. Well, that’s cheating… right 2slug?
No, it’s “cheating” when your protocol doesn’t set up a properly constructed control group. The problem with their study isn’t that the doses differed from other studies; the problem is that they didn’t establish rigorous controls over the two groups in their own study.
And what is the point of mentioning the German findings? What does that have to do with hydroxychloroquine?
Have you ever done any actual statistical studies? It doesn’t sound like it.
Bruce Hall, why do you cite studies when you do not understand them?
” then that ought to count as a COVID-19 death just as much as if the person died directly from COVID-19.”
Not if it was a government policy that caused the inability to see the doctor.
sammy I am not aware of any government policy that prevented hospitals and EMTs from responding to heart attacks and strokes. The stories in Bruce’s link were about people who made a conscious decision not to seek help when they should have out of fear of catching COVID-19.
sammy is simply making up excuses for team trumps follies.
Huh? What does that mean? If the ICU is full or might be due to COVID outbreaks and the government, federal or local, has to deal with it, you are saying that does not count? Your logic is beneath contempt.
You actually have a point in your own weird way. People are dying in incredible numbers because of the chaotic policies emanating from our White House. Oh wait – Sammy adores Trump. So it is the policies of Sammy’s favorite policies that are leading to all these deaths. Great job Sammy!
“This approach is not persuasive if you thought the excess deaths were primarily people who were going to die in the very near future”
Ah, but those people are already accounted for in the dotted line – expected number of deaths.
Maryland2: Well, near future is outside of the window being analyzed – so maybe dying today instead of 1 year later…
@ Menzie
I thought you might take an interest in this Sir. I know you read NYT semi-regular but on the small chance you missed it. The paper referenced is linked inside the article.
https://www.nytimes.com/2020/06/30/upshot/coronavirus-economists-dexamethasone.html
Is Donald Trump reading Bruce Hall’s incredibly stupid comments?
https://www.reuters.com/article/us-health-coronavirus-usa-trump/trump-again-hails-u-s-covid-19-testing-as-cases-rise-by-record-levels-idUSKBN2440FK
“There is a rise in Coronavirus cases because our testing is so massive and so good, far bigger and better than any other country,” Trump said in a tweet late on Thursday. “This is great news, but even better news is that death, and the death rate, is down,” he said.
More people with this virus is good news only to the dumbest person ever. But then again – this is what Bruce Hall keeps telling us. I learned about this pathetic tweet watching Morning Joe mock it thoroughly. If they could only read the intellectual garbage posted here by Bruce Hall!
I’m listening to Peter Navarro on MSNBC right now and I do declare he has gone bonkers. First he attacks China for giving us “weaponized” coronavirus and then he attacks Dr. Fauci for some bozo reasoning. I’m sure this would give Bruce Hall a woody but what is going to get Brucie all excited is something coming out of a Detroit hospital:
https://www.cnn.com/2020/07/02/health/hydroxychloroquine-coronavirus-detroit-study/index.html
Study finds hydroxychloroquine may have boosted survival, but other researchers have doubts
Of course nutcase Navarro does not mention the doubts. No this clown is still trying to sell this snake oil as the miracle cure.
https://twitter.com/drdavidsamadi/status/1279044039950639104
Go for it p.
Bruce Hall: Why should we give credence to a urologist, who had to settle a fraud case brought by USA Geoffrey Berman?
Bruce Hall is still pushing Hydroxychloroquine? Why would we give credence to any one Bruce Hall cites? Most of his ‘experts’ are fraud and in the once in the Blue Moon situation where he links to a reliable source, he misrepresents what it says. And he claims we are not bringing actual data to the discussion. Seriously?
There has been enough study of hydroxychloroquine now, if it was a beneficial therapeutic it would have clearly shown by now. Given the lack of any positive outcomes, its best to move on to more promising prospects.
Peter Navarro just today told us that hydroxychloroquine was a very effective treatment. He also revealed he is sitting on a bunch of this stuff which he wants to sell us for big bucks!
No, that’s not exactly a scientific approach. How many iterations of a light bulb did Edison make before he found an effective “protocol”?
I would have expected more from you. Just because one light bulb didn’t work doesn’t mean a properly constructed light bulb wouldn’t work. Likewise with testing and medical protocols.
https://twitter.com/drdavidsamadi/status/1279082359514525696
You can skip up to around 13 minutes if you are impatient.
Statistically if u you continue to run uncontrolled studies, one is bound to show some positive outcomes. Should that one study outshine the other 100 studies that show neutral or negative outcomes? If hydroxychloroquine were a “game changer”, it would show as the dominant outcome even in these uncontrolled studies. It does not. And it has shown ineffective even in controlled studies. Time to move on bruce. We need to spend our time and resources on something that will be effective and game changing. I understand its an ego thing and you simply cannot admit wrong, but you are.
“Bruce Hall
July 3, 2020 at 1:38 pm
pgl,
your lack of thoroughness is my dishonesty?”
This is rich from the troll who reads the title of his own link and then goes off on some stupid conclusion contradicted by the rest of the discussion in his own damn link. Bruce – you have been caught doing this 1000’s of times. Now which is it? Are you too stupid to read your own links? Or do you know you misrepresent even your own links. Is it stupidity or mendacity? In your case – BOTH!
57000 new cases of cOVID19 just today breaking yesterday’s daily record of 52000 new cases. But the Idiot in Chief declares this to be good news? After all our testing is the best in the world – even though it is not. And of course no one is dying – yet. So it is all grand.
Where does Trump get this BS? Well right here as this is what Bruce Hall keeps telling us over and over again. Go figure.
2slug had a nice summary of the incessant nonsense from Bruce Hall earlier today:
“So let’s review some of your claims surrounding the COVID-19 virus:
(1) You assured us that it was no worse than the flu. You were wrong.
(2) You were confident that it was seasonal and would go away with warmer temperatures. You were wrong.
(3) You claimed that hydroxychloroquine was an effective treatment for COVID-19. At best your claim is unproven. At worst it’s outright wrong and dangerous.
A few days ago you indicated that you don’t wear a mask.”
One wee problem with this. It is as if Brucie boy came up with all of this disproven claims on his own. Bruce Hall doing independent thinking? REALLY? Note how perfectly this nonsense correlates with the lies etc. from Donald John Trump. OK maybe Bruce is not Trump’s minnie me. Could it be that Donald Trump comes up with nonsense reading Bruce Hall’s really stupid comments?