Suppose the historical correlations between the 7 day moving average of covid deaths and hospitalizations and ICU beds holds. What does that imply for future trends in covid related deaths?
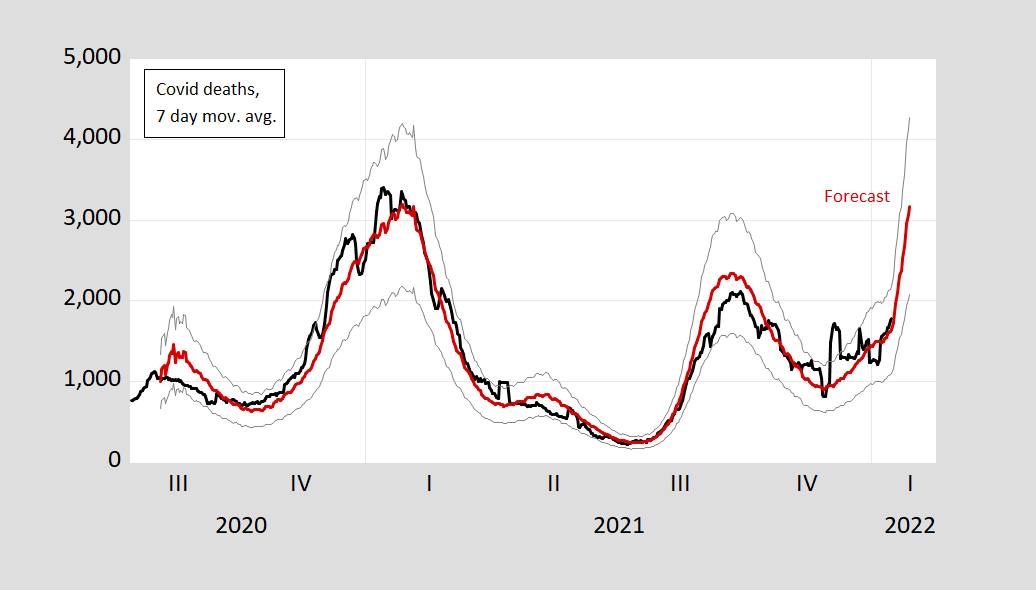
Figure 1: Covid deaths, 7 day moving average (black), and prediction based on log-levels OLS regression 7 day moving average of deaths on lagged hospitalization and ICU (red), 95% confidence interval (see text below). Source: Our World in Data accessed 1/16/2022, author’s calculations.
Point estimate of 3176 deaths (7 day moving average) on 1/28.
I used the sample 8/5/2020 to 1/15/2022, to estimate:
ldeathst = 357.08 + 0.816lhospt-21 + 0.300 licut-14 – 0.054trend + 0.000002trend2
Adj R2 = 0.94, SER = 0.165, DW = 0.09, N=529, bold denotes significance at 5% msl, using HAC robust standard errors.
This ad hoc specification is drawn on the following observations:
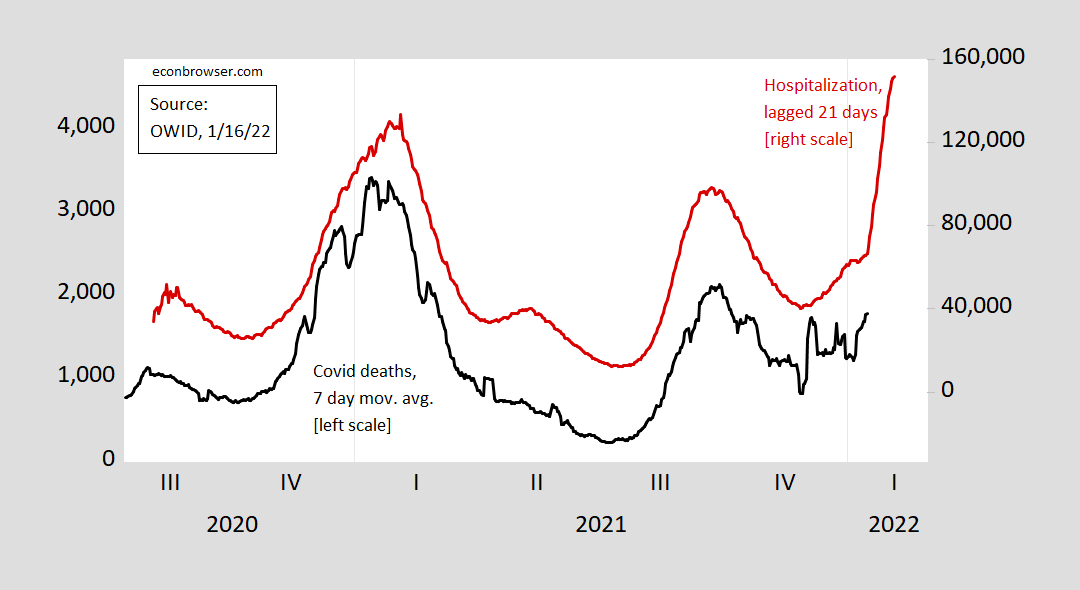
Figure 2: Covid deaths, 7 day moving average (black, left scale), hospitalizations lagged 21 days (red, right scale). Source: Our World in Data, accessed 1/16/2022.
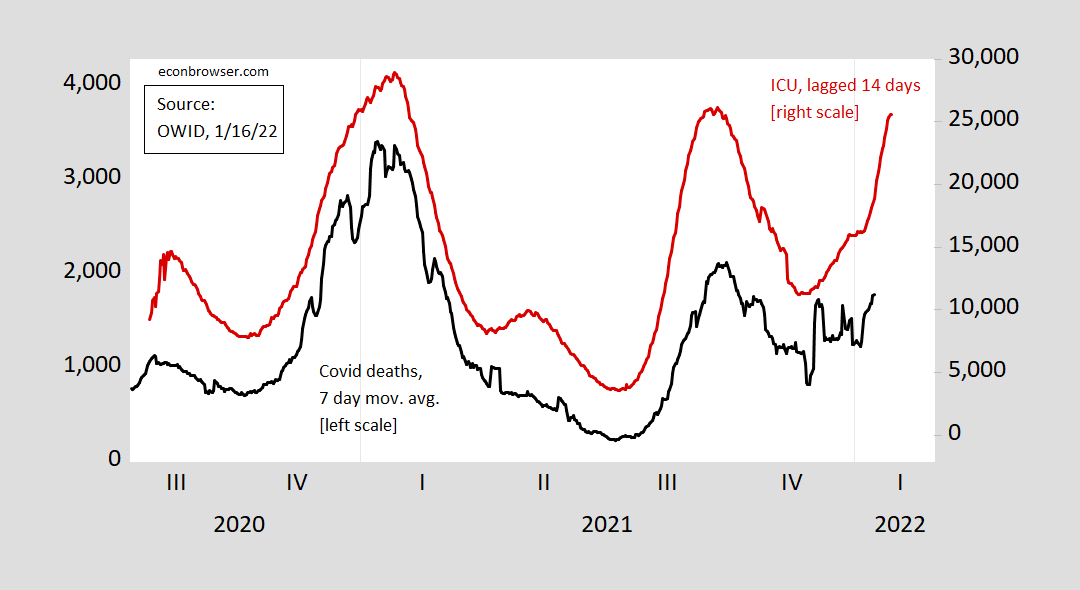
Figure 3: Covid deaths, 7 day moving average (black, left scale), ICU use lagged 14 days (red, right scale). Source: Our World in Data, accessed 1/16/2022.
Since the in-log-levels specification exhibits a high degree of serial correlation (possibly a spurious regression), then I estimate in first differences.
Δldeathst = 0.00045 + 0.276Δlhospt-21 + 0.270Δ licut-14
Adj R2 = 0.07, SER = 0.048, DW = 1.69, N=529, bold denotes significance at 5% msl, using HAC robust standard errors.
(The coefficient on a linear time trend is not statistically significant.)
This specification yields lower forecast, 2342 at 1/28, which would come close to the Fall 2021 peak (9/30).
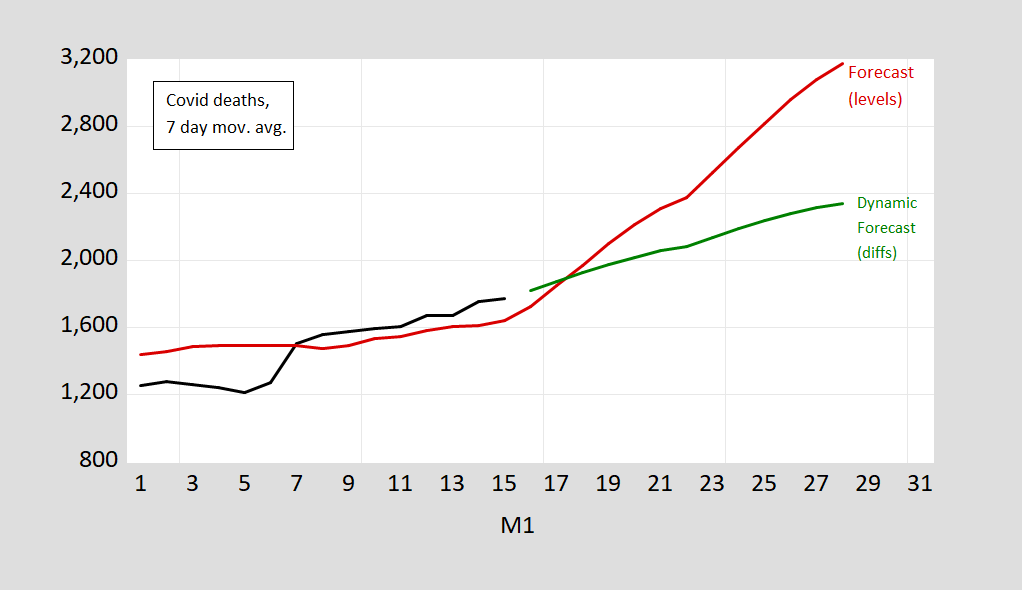
Figure 4: Covid deaths, 7 day moving average (black), and prediction based on log-levels OLS regression 7 day moving average of deaths on lagged hospitalization and ICU (red), and based on first differences of logged values (green) (see text above). Source: Our World in Data accessed 1/16/2022, author’s calculations.
It’s too soon to sort through the effects that determine the lethality of Omicron. If vaccination has differing effects on infection, hospitalization and death across different variants, the correlation between series will change. It would be lovely if Omicron proves less deadly overall and that vaccines provide strong protection against severe cases. That’s the narrative that has developed in the press. Your first-difference model looks like a simple test of the received narrative.
Is the modification of human behavior the reason for the dramatic drop in the 7-day moving averages from the peaks (not now obviously, but when they have happened in the past)?? That strikes me as rather odd (although I do tend to believe these numbers) and not something i would have foreseen “intuitively” before the virus hit.
One of the reasons I ask this is IHME is forecasting a dramatic drop in both infections and hospital bed usage by March, and I was tempted to call bullsh*t before looking at how the prior peaks dropped so quickly.
The answer the question in the 2nd sentence may very well be “not nearly as much as it once did”. It will be interesting to see how this plays out but I wouldn’t be surprised if these prior correlations fail to hold given how experts have suggested “Omicron is a dud” (sorry, I couldn’t resist) relative to prior strains when considering virulence. Moreover, the suggestion that Omicron is much more highly transmissible, we can see hospitalizations skyrocket even if a lot of COVID hospitalizations aren’t actually due to COVID. I know many healthcare systems have improved their reporting and some distinguish between “with COVID” and “because of COVID” but I do not believe the reporting has been standardized across systems/states/you name it. Additionally, to the correlation question, vaccines should lower deaths. There has been a ton of talk on decoupling between cases:outcomes as well as hospitalization:death with Omicron. As I said in another thread, the strain of people out of work, etc could very well have the ?worst/largest aggregate impact on the US just as the northeast has been experiencing recently.
Menzie,
Well, given the apparently weakened deadliness of the omicron variant compared to the precious ones, then a correlation based on the previous variants might not hold so well. That said, there probably is some correlation, and the lag might be about right, although that could change too. Without doubt, deaths follow hospitalizations by some period of time, although that could vary across variants.
Watching “The French Dispatch” on disc right now. My Dad loved newspapers, so you know I had to watch this. What’s really weird about this is, it seems to take place (at least partly) in Liberty Kansas, and I used to live not but about an hour’s drive from there. Kinda weird. Like many of Wes Anderson’s pictures, so far has a strong nostalgic quality to it.
An interesting wild card in the equation:
https://www.detroitnews.com/story/news/world/2022/01/17/israel-study-4th-vaccine-shows-limited-results-omicron/6556865001/
If the vaccines have very limited effect on the Omicron variant (even after the 4th booster), then we had better hope that the variant has a much lower natural lethality.
Now if you actually finished reading your own link, you might have noticed:
‘Israel’s aggressive vaccination efforts have not been able to stop an omicron outbreak in recent weeks. The variant has caused record-setting infection levels and sent a growing number of people to the hospital, though the numbers of seriously ill remain below previous waves.’
More cases may indeed not lead to more deaths among the vaccinated. Of course wearing one’s mask is still prudent.
Yes, that’s in the article. What isn’t in the article is an assessment of the virus itself.
Are people not dying because the vaccinations are effective and the study indicating they are quite ineffective is flawed? Or are the vaccines ineffective as the study indicated, but the virus is a much milder strain and people are getting in and out of the hospital quickly? Your statement seems to indicate the former in your opinion. This might indicate the latter: https://news.yahoo.com/cdc-walensky-cites-study-showing-173151295.html
Yes, If you wear a tight fitting N95 mask you will benefit, especially if the variant circulating nearby is Delta; if you wear anything else, it is likely virtue signaling.
https://www.kwtx.com/2022/01/08/health-experts-warn-cloth-masks-are-ineffective-against-covid-19/
Bruce Hall Well, one way to resolve this is to compare outcomes between vaccinated and unvaccinated individuals. While it’s almost certainly true that the omicron variant is inherently less lethal than the delta variant, that doesn’t mean both populations are equally protected. It’s still true that most of the very serious cases that put people in a hospital bed or a coffin are among the unvaccinated even though the unvaccinated represent a minority of the overall population. I find it amusing how the same people who pooh-poohed the seriousness of the delta variant as being nothing more than the flu are not emphasizing how much more deadly the delta variant was than the omicron variant.
Over the holidays my nephew’s wife, who is a COVID nurse at Mayo, and my brother’s wife, who is a researcher at university hospital, were talking about some of the effects they’re finding among those who survived even mild cases of COVID. It’s not just a loss of smell, which reflects how the virus attacks the brain. The virus also seems to be targeting the pancreas and liver, which in turn is causing diabetes. Even worse, they’re finding sharp increases in the recurrences of cancers that had been in remission.
That would be an interesting study if the data were available. Too much anecdotal information being bounce around. It would be especially interesting for the 65+ demographic since a large majority of those have been “fully vaccinated”. That demographic is the most vulnerable.
What we are seeing now are increases in children with fevers being admitted to the hospital, although children had cases and fevers before, but the most seriously ill were the elderly which used most of the hospital resources at the time. Virtually all of them are discharged in the minimum time hospital policy (and government reimbursement) allows… regardless of vaccination status.
A lot of resources have been wasted on the very young where the vaccinated/unvaccinated status is essentially meaningless in terms of serious outcomes. Rather, the strategy should have shifted a year ago to antivirals. Pfizer is about to release its version.
https://www.weforum.org/agenda/2021/12/covid-19-pill-pfizer-cure-effective/
“These are very exciting results,” Paul Sax, a professor at Harvard Medical School, told Reuters.
If this strategy had been employed early on and targeted for the most vulnerable first, it would have accomplished three things:
1) a reduction of serious illness and deaths among the elderly who comprise over 80% of COVID deaths
2) the anti-viral mechanism would have a broader effectiveness than the current vaccines which have limited impact on Omicron
3) the medication could have been distributed in advance so that anyone testing positive could have taken it as needed and not strained our medical system.
A potential fourth benefit would have been the emergence of even better anti-virals as resources and attention was directed there instead of booster shots of limited effectiveness vaccines.
It’s admirable effort, but still very speculative.
1. Omicron is a very different variant than Delta (or alpha, beta), especially in terms of per case impact. So training the model on earlier Covid has some real uncertainty here.
2. In particular, the model is trained only with US observed lags (fine, since we’re looking at US to come, but then you’re not capturing insights from other countries where Omicron has swept through. Seemingly this info ought to affect a Bayesian prediction somehow.
3. Recent (DEC) data may be heavily contaminated with Delta, but that is changing to Omicron very rapidly. So DEC may not drive JAN.
4. Even if it were exactly same Covid, population is different.
5. I am way out of my depth in econometrics, but just based on knuckle dragger six sigma manufacturing consulting:
A. I think a lot of your model is driven by trend and trend squared. Essentially trying to predict a parabola. But really, realize you’ve got very low degrees of freedom in predicting parabolas, since you’ve had a couple previous parabolas. I think this is something in time series analysis, where people end up getting confused by the mass of individual observations, but lose sight of the number of trends observed. I’ve seen a lot of parabolas predicted in the peak oil community and not do that well, if they were predicted during the ramp (i.e. before turning).
B. The other thing is it seems like the regression is more driven by hospitalization than ICU. Which doesn’t make sense intuitively, given that ICU is a lot closer to death than hospitalization.
Anonymous: (5.A) Take out the trend and trend-squared and adjusted R2 is unchanged. (5.B) In levels, you are right “beta”-coefficients (scaled by standard deviations) for hospitalization has bigger effect. In differences, they’re about the same effect. If I believe the latter specification, then that’s the right comparison.
5A.
1. I wouldn’t add extra terms if they don’t drive a significant improvement in the Rsq. Keep it simple.
2. How much does the future outcome change by omitting those terms? Do you get the same peak timing, amount?
Israel is an interesting case study. They were hailed as leaders early in 2021 when they secured large numbers of early vaccine doses and had rapid uptake. But that has stalled. There are a lot of (mostly young) anti-vaxers in Israel such that today they actually have an lower total vaccination rate than the even the dismal U.S. rate.
Israel is seeing a skyrocketing number of cases but so far not a very big increase in deaths. Presumably this is because they have had pretty good vaccine compliance among the elderly over age 60.
So we may see something similar in the U.S. Lots of cases and short term hospitalizations but fewer severe ICU cases and deaths. The vaccines work.
For me, looking at this Israel question, I think of the Economic idea “decreasing returns to scale”. If the virus hasn’t changed that much, what are you getting back on that 4th vaccine?? I would argue unless that 4th vaccine is very strongly tailored/designed to weaponize for that new/specific variant, you’re just not gonna get a whole helluva lot out of that 4th shot. But I have zero background in epidemiology or public health……. so take it for what it’s worth.
https://www.voanews.com/a/eu-drug-regulator-warns-against-overuse-of-covid-booster-shots/6395174.html
If the level of antibodies and T-lymphocyte immunity is getting lower with time and an additional booster can get them higher (above a presumed threshold that provides “protection”) you could make the case for using them. Its my understanding that this is the case for antibodies, but T-lymphocytes (and the important subset of helper T-lymphocytes) seems to hold up pretty well after the third shot of RNA vaccines. The scientific case for a 4’th shot of RNA vaccines to the general public is pretty weak at this time.
Israel reports number of vaccine doses administered, but not number of residents vaccinated. Looking to number of doses administered, however, over 90% of residents have been fully vaccinated which would mean a theoretical herd immunity level has been reached by Israel. There are currently many infections, but almost no new deaths:
https://www.worldometers.info/coronavirus/
January 16, 2022
Coronavirus
Israel
Cases ( 1,792,137)
Deaths ( 8,318)
Deaths per million ( 892)
https://graphics.reuters.com/world-coronavirus-tracker-and-maps/countries-and-territories/israel/
January 17, 2022
Israel…
Because Omicron is so very infectious it is hitting the big cities (NYC and DC) very early and hard. But those are also places with higher rates of vaccination. As the virus moves into less populated and less vaccinated areas we may find that overall lethality goes up. I expect to be surprised sometime in the next month.
Further complicating the issue of figuring out Omicron, is the fact that a substantial % of cases (and particularly deaths), even now, may be from Delta. We don’t do nearly enough sequencing to allocate individual deaths to either Delta or Omicron.
https://www.worldometers.info/coronavirus/
January 17, 2022
Coronavirus
New York
Cases ( 4,665,446)
Deaths ( 62,465)
Deaths per million ( 3,211)
Chinese coronavirus vaccines began to be administered on the mainland on an emergency basis in June 2020. General administration according to infection vulnerability began in December 2020. More than 2.93 billion doses have been administered so far, with more than 1.22 billion mainland residents now fully vaccinated. There has been “no death” of a fully vaccinated mainland resident. Since June 2020, there have been only 2 coronavirus deaths in mainland China.
However, those Chinese vaccines are remarkably more effective when administered in China than when administered in other countries (with independent health monitoring), I makes you wonder if the Chinese have consulted with DeSantis on how to get good numbers.
“There has been “no death” of a fully vaccinated mainland resident. Since June 2020, there have been only 2 coronavirus deaths in mainland China.”
This has nothing to do with the vaccine. You have very little data from the Chinese mainland that measures the efficacy of the vaccine.
ltr: “Israel reports number of vaccine doses administered, but not number of residents vaccinated. Looking to number of doses administered, however, over 90% of residents have been fully vaccinated which would mean a theoretical herd immunity level has been reached by Israel.”
Taking total doses and dividing by two, as you did, gives a misleading number in Israel because a large portion of the double vaccinated have had third doses. Various sources both in and out of Israel put the vaccinated population somewhere around 70% to 74%, which is below the U.S. There’s a lot of vaccine hesitancy, particularly among Orthodox Jews, Arabs, and also a very low rate of vaccination for those between 5 and 12 years. More than a third of Israelis are under age 18 and these are the least vaccinated.
So no herd immunity (yet) and hence the huge increase in infections, more than three times all previous peaks. Cases per 100,000 is similar to the spike in the U.S. But deaths are holding steady at low numbers, so that bodes well for the U.S.
Taking total doses and dividing by two, as you did, gives a misleading number in Israel…
[ Likely this criticism is correct, and there has been vaccine hesitancy in Israel, but the number of vaccine doses administered is so high relative to residents and previous deaths so shaking that I argued for a higher portion of fully vaccinated. I accept your criticism.
https://graphics.reuters.com/world-coronavirus-tracker-and-maps/countries-and-territories/israel/
January 17, 2022
Israel has administered at least 17,626,777 doses of COVID vaccines so far… ]
If you go to your own link, click on “See our new vaccination tracker” and then scroll way down to Israel, you will see 73%.
If you go to your own link, click on “See our new vaccination tracker” and then scroll way down to Israel, you will see 73%:
https://graphics.reuters.com/world-coronavirus-tracker-and-maps/countries-and-territories/israel/
[ Thank you so much:
The Vaccination tracker lists fully vaccinated in Israel at “66.5%” and single dose vaccinated at 73.7%. A fully vaccinated rate of 66.5% in Israel is far lower than I had estimated from just reading the doses administered.
I do appreciate the correction. Thank you, again. ]
Israel
66.5% fully vaccinated
73.7% vaccinated with at least a single dose
17,626,777 doses of COVID vaccines administered
9,326,000 population
https://www.jpost.com/health-and-wellness/coronavirus/article-693836
January 18, 2022
As of Tuesday, the Health Ministry had not released complete updated data on the pandemic trends in Israel since Sunday night due to technical problems.
There were 65,259 new cases on Monday and 62,210 on Sunday, it said. The previous highest number, registered last Wednesday, was 48,095.
There were 498 patients in serious condition, including 100 on ventilators and 13, the most critical cases, on extracorporeal membrane oxygenation machines (ECMO). Last Tuesday, there were 219 patients in serious condition.
https://www.jpost.com/health-and-wellness/coronavirus/article-693836
January 18, 2022
COVID-19: New daily infections record of 65,259 in Israel
New cases reach record of 65,259 • Decision to shorten quarantine was made to “find a balance between medical and social needs”
By ROSSELLA TERCATIN
Israel should cancel its Green Pass system, Finance Minister Avigdor Liberman said Tuesday as the country registered a record 65,259 new coronavirus cases.
He made his remarks a few hours after he, together with Prime Minister Naftali Bennett and Health Minister Nitzan Horowitz, said more than 25 million at-home antigen tests would be distributed free to Israelis in the upcoming days.
“There is no medical and epidemiological logic in the Green Pass as many experts concur,” Liberman wrote on Twitter. “What there is, is a direct damage to the economy, daily functioning and in addition, a significant contribution to panic among the public. I am working with all parties to eliminate the Green Pass and preserve a normal routine for all of us.”
Under the Green Pass outline, only people who are vaccinated, recovered or tested in the previous day – or 72 hours in specific cases – can access certain activities and venues, and in some instances, their workplace.
With the rise of the Omicron variant, the number of breakthrough infections and reinfections (individuals catching the virus despite being vaccinated or recovered) has skyrocketed.
Health officials and experts, including Health Ministry Director-General Nachman Ash, have said inoculation and recovery still offer some degree of protection, and therefore the Green Pass system should be kept in place. However, they also acknowledged that at some point the question might need to be reexamined….
Yes, If you wear a tight fitting N95 mask you will benefit, especially if the variant circulating nearby is Delta; if you wear anything else, it is likely virtue signaling.
[ Importantly the Chinese apart from medical personnel invariably wear blue-woven masks, with a particular exception being when members of the foreign ministry are with international visitors. The success of the Chinese in limiting infections suggests the blue-woven masks are effective. As for virtue signaling, I find the expression offensive. I am comforted by blue-woven mask wearers and wear the same to comfort others. ]
I would comfortably go with the level equation here. I would not concern myself with spurious correlation as there is a clear-cut theoretical link between hospitalizations, ICUs and deaths. I would be reluctant to difference the data (in this particular regression) for several reasons. First, eyeballing the level series and imagining it in differences, it looks like differencing would throw out a lot of the signal and stress the noise and the measurement errors (I’m looking at the high freq. wiggles in the red and the black lines). We don’t want to model noise and measurement errors. Second, the level equation coeffs look sensible. Third, the regressors are lagged and the “true” lag is unknown. Changing the time lag for a day or so would likely leave the level equation intact whereas the equation in differences is likely to be very sensitive to this change. Excess ac in the level equation is concerning but we’ve got se estimators that can deal with it better than differencing does.
a couple hours ago i went over to “theHill.com” to see if there was any DC news i should be following up on, certainly not looking for any Covid or vaccine news over there….but these are the Covid related articles i came across since, without even trying…
Milley tests positive for COVID-19 – Chairman of the Joint Chiefs of Staff Gen. Mark Milley tested positive for COVID-19 on Sunday and is isolating. Col. Dave Butler, spokesperson for the Joint Staff, said in a statement that Milley is experiencing “very minor symptoms” and can perform his duties remotely. Butler said Milley is fully vaccinated against the coronavirus and has received a booster vaccine dose. All other Joint Chiefs of Staff, except for one, tested negative for COVID-19. Officials have not said who that one was. . Also on Monday, the Marine Corps announced that its Commandant Gen. David Berger tested positive for COVID-19. “The performance of his duties will remain unaffected,” commandant spokesperson Maj. Eric Flanagan said in a statement to The Hill. Milley and Flanagan are the latest top Defense officials to test positive for COVID-19 this month. Defense Secretary Lloyd Austin announced on Jan. 2 he had tested positive. He also experienced mild symptoms and worked remotely.
Colorado Democrat latest House member to test positive for COVID-19 – Rep. Diana DeGette (D-Colo.) on Monday announced she had tested positive for a breakthrough case of COVID-19. “I have tested positive for COVID-19. Thankfully, I am fully vaccinated and boosted and experiencing mild symptoms,” DeGette’s announcement comes as the latest coronavirus surge, driven largely by the omicron variant, sweeps through Congress. At least 14 members of the House and one senator tested positive for coronavirus this month, including Reps. Alexandria Ocasio-Cortez (D-N.Y.), Jim Cooper (R-Tenn.), Sean Casten (D-Ill.) and Young Kim (R-Calif.). Overall, there have been at least 50 breakthrough cases of COVID-19 among vaccinated members of Congress since last summer. More than half of those breakthrough cases have been since mid-December. Iowa Rep. Ashley Hinson (R) announced Friday that she had tested positive for the virus a second time within two years. “Yesterday afternoon, I began experiencing mild, cold-like symptoms. I took a COVID-19 test and the results were positive. I am fully vaccinated and boosted against COVID-19,” Hinson wrote in a tweet.
Maryland Democrat announces positive COVID-19 test – Rep. David Trone (D-Md.) announced he has tested positive for COVID-19 in the latest breakthrough case among lawmakers in Congress. “Today, I tested positive for COVID-19. I’m fully vaccinated + boosted, and am only experiencing mild symptoms,” Trone wrote in a tweet on Saturday. “I’ll be voting by proxy this week. Trone’s infection follows similar announcements in the past week or so from Reps. Dutch Ruppersberger (D-Md.), Alexandria Ocasio-Cortez (D-N.Y.), Jim Cooper (R-Tenn.), Sean Casten (D-Ill.) and Ashley Hinson (R-Iowa.). Rep. Diana DeGette (D-Colo.) also announced she has tested positive for COVID-19 in a tweet on Monday, adding she is experiencing mild symptoms. “I have tested positive for COVID-19. Thankfully, I am fully vaccinated and boosted and experiencing mild symptoms,”
Preliminary Israeli study shows fourth vaccine not enough to stop omicron– A preliminary study in Israel, believed to be the world’s first, found that a fourth COVID-19 vaccine is not enough to prevent omicron infections. Gili Regev-Yochay, director of Sheba Medical Center’s Infectious Diseases Unit, said the trial studied the effect of the Pfizer booster after two weeks and the Moderna booster after one week, according to Reuters. Regev-Yochay said the increase in antibodies from a fourth shot was “probably not enough for the Omicron.””We know by now that the level of antibodies needed to protect and not to got infected from Omicron is probably too high for the vaccine, even if it’s a good vaccine,” she added.Sheba Medical Center ran the trial on second booster shots among 150 of its staff members, and its findings were preliminary and unpublished,The Times of Israel reported. About 500,000 Israelis have been inoculated with a fourth dose as of Sunday.Israel has led the push for vaccinations throughout the pandemic and was the first country to begin to offer booster shots to its population.Prime Minister Naftali Bennett previously announced that the country would begin offering a fourth vaccine as a second booster shot for high-risk populations and vulnerable groups. Despite the push for vaccinations, Israel reported nearly 12,000 new COVID-19 cases earlier this month, a record-setting figure for daily case rates since the start of the pandemic.“There is no control of the omicron wave,” Sharon Alroy-Preis, the Israeli health ministry’s top public health official, said to a local news outlet at the time.
https://news.cgtn.com/news/2022-01-18/Chinese-mainland-records-171-confirmed-COVID-19-cases-16UO2Q3gTXG/index.html
January 18, 2022
Chinese mainland reports 171 new COVID-19 cases
The Chinese mainland recorded 171 confirmed COVID-19 cases on Monday, with 127 linked to local transmissions and 44 from overseas, data from the National Health Commission showed on Tuesday.
A total of 33 new asymptomatic cases were also recorded, and 760 asymptomatic patients remain under medical observation.
Confirmed cases on the Chinese mainland now total 105,258, with the death toll remaining unchanged at 4,636 since January last year.
Chinese mainland new locally transmitted cases
https://news.cgtn.com/news/2022-01-18/Chinese-mainland-records-171-confirmed-COVID-19-cases-16UO2Q3gTXG/img/ac09be7b518040b9a0484613a69dc81d/ac09be7b518040b9a0484613a69dc81d.jpeg
Chinese mainland new imported cases
https://news.cgtn.com/news/2022-01-18/Chinese-mainland-records-171-confirmed-COVID-19-cases-16UO2Q3gTXG/img/ecb60cf1cc534f1c95e5a8c2e47e8eb1/ecb60cf1cc534f1c95e5a8c2e47e8eb1.jpeg
Chinese mainland new asymptomatic cases
https://news.cgtn.com/news/2022-01-18/Chinese-mainland-records-171-confirmed-COVID-19-cases-16UO2Q3gTXG/img/63d23ddff5914e89bcee93e55da5ef72/63d23ddff5914e89bcee93e55da5ef72.jpeg
https://news.cgtn.com/news/2022-01-18/Chinese-mainland-administers-over-2-94b-vaccine-doses-16VBLVZgcGQ/index.html
January 18, 2022
Chinese mainland administers over 2.94b vaccine doses
The Chinese mainland had administered more than 2.94 billion COVID-19 vaccine doses as of January 17, according to data released by the National Health Commission.
[ January 15, 2022
Over 1.22 billion fully vaccinated against COVID-19 on Chinese mainland. ]
https://www.worldometers.info/coronavirus/
January 17, 2022
Coronavirus
United States
Cases ( 67,631,191)
Deaths ( 874,321)
Deaths per million ( 2,618)
China
Cases ( 105,087)
Deaths ( 4,636)
Deaths per million ( 3)
past time to observe vaccines, etc have not returned us’ excess deaths to pre covid pandemonia levels.
attributing the vaccines to anything has more consumer risk that the fda test procedure.