Or, the GOP plan to eliminate the surplus population
From CBO:
CBO and JCT estimate that enacting this legislation would reduce the cumulative federal deficit over the 2017-2026 period by $321 billion. That amount is $202 billion more than the estimated net savings for the version of H.R. 1628 that was passed by the House of Representatives.
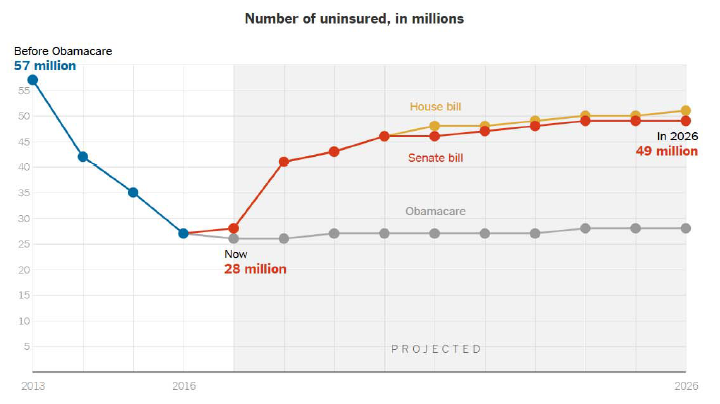
The Senate bill would increase the number of people who are uninsured by 22 million in 2026 relative to the number under current law, slightly fewer than the increase in the number of uninsured estimated for the House-passed legislation. By 2026, an estimated 49 million people would be uninsured, compared with 28 million who would lack insurance that year under current law.
Here is a time series plot of the number of uncovered under the Senate bill (the Better Care Reconciliation Act of 2017), the House Bill, and current Law.
A substantial component of the entire plan involves reducing spending for Medicaid relative to current law baseline (which :
By 2026, among people under age 65, enrollment in Medicaid would fall by about 16 percent and an estimated 49 million people would be uninsured, compared with 28 million who would lack insurance that year under current law.
One way to think about the overall project is that Medicaid spending (which benefits primarily lower income households) is slashed by $772 billion in order to finance $541 billion of tax cuts, the bulk of which will go to high income households. In this sense, the plan is entirely consistent with Republican policy measures proposed in recent years, so kudos for consistency of goals. The redistribution is illustrated in CBO Figure 1.
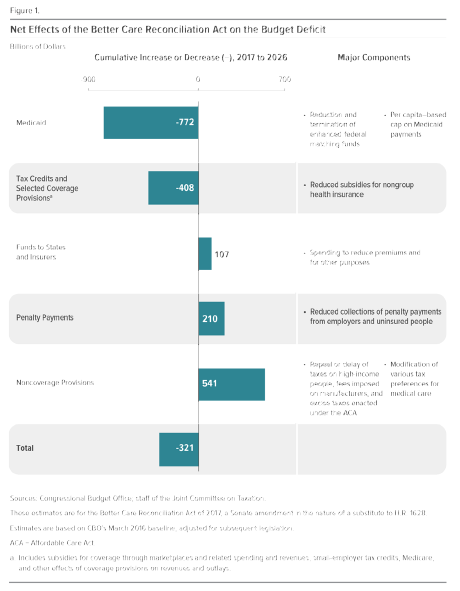
Source: CBO, 26 June 2017.
Given the reduction in coverage of non-elderly adults by 2026 is 22 million, we can use the estimates provided by Center for American Progress to judge that mortalities will be elevated by about 207.5 thousand (cumulative) over the next decade, and deaths in 2026 elevated by about 26,500. In this context, the title of the Senate “Better Care Reconciliation Act” (I think “bitter” is more apt) is truly Orwellian.
I wonder if Paul Ryan is embarrassed that his bill insures 1 million less people *and* costs $119 billion more.
I’m just kidding, he’s absolutely not embarrassed.
“the GOP plan to eliminate the surplus population”. Exactly. But hey – these “moochers” vote for Democrats so getting rid of them is good for McConnell and Ryan.
Imagine if a plane with 500 people on board crashed. There would be massive investigations to see what went wrong and there would be no limit to the cost we would spend to make sure it doesn’t happen again. Now, imagine if that happened ever week and Congress & the President were OK with it.
THAT is what the Republicans are doing with this bill.
Sick. Sad. Mean.
U.S. mortality rates were predicted to fall after Obamacare. Instead, they surged, most likely due to the economic depression, expensive insurance, high deductibles, and doctors not accepting new patients.
Medicare and Medicaid bankruptcies won’t help.
God, you are an absurd person.
Suicide rates, alcoholism, and opiods increases mortality.
And, don’t forget too much sugar 🙂
Would you give us a source for this claim?
Also, life expectancy fell under Obamacare.
http://thefederalist.com/2017/04/25/running-numbers-mortality-rates-suggests-obamacare-killing-people/
This is probably one of the most idiotic references you’ve posted yet. It just recycles old garbage that’s been disproven many times over. Zombie facts. Since you seem to have time to surf the web all day, why don’t you do a little independent research and find out why those claims happen to be false.
The other problem with your post is that increasing lifespans is only one reason people should have health insurance. Most people use health insurance for serious but not life threatening ailments.
Studies show Obamacare turned-out to be much worse than predicted:
https://www.google.com/amp/legalinsurrection.com/2017/02/study-contrary-to-dem-claims-repealing-obamacare-will-not-increase-mortality-rates/amp/
You really struggle with cause-and-effect, huh?
When it comes to poor government policy, people like you ignore the biggest cause, and blame everything else.
Some true predictions:
“The Economic Policy Journal predicted in 2012 that “life expectancy will decline under Obamacare.” In 2009, the dean of Harvard Medical School, Jeffrey Flier, predicted that Obamacare would cost lives by harming life-saving medical innovation. In 2013, two doctors wrote in The Wall Street Journal that Obamacare is “bad for your health,” and that it would eventually have a devastating effect on medical innovation by driving down investment in medical devices.”
I seem to remember the Republican candidate promising a far better, far cheaper, far more inclusive replacement for Obamacare that would cover everybody. No cuts to Medicaid either. He took special pride in being the only Republican making those promises.
And the congressional Republicans? Forgive them, Father, they know not what to do because they’ve only had seven years to figure out what TO DO. These days, who can really think of anything in 84 months?
Ah, ancient history. These days, even a year is such a long time.
The data shows that the reason the death rate was up last year was a huge surge in automobile accident deaths.
Would you please explain how Obamacare caused auto accidents to jump.
Obviously, you either didn’t read or understand the link above.
Let’s go single payer system – better yet, let us all adopt California’s SB 562 single payer system, and be done with it, so that nobody is left behind. California put it on hold for a while, but I think we can adopt it at the federal level, and bring security, certainty, prosperity and happiness to all.
Since we are at it, we should adopt single payer for everything – single payer cars, single payer banking, single payer air conditioning, single payer food, single payer clothing, single payer housing, single payer education, all single payer throughout. We all pay a small fee to the government (the single payer user fee), and the government will provide us with all our needs, and some wants. But those wants are not needs, so they are not important – the government will decide, of course, because they are best at deciding – better yet, the CBO, since it is non-partisan (as always stressed by Menzie), should decide what is a “need” and what is a “want”. That is the new scoring assignment for the CBO. To decide exactly what I really need and what I merely want – that is, I and 300 million other people. The CBO employs smart people, all PhDs, probably many from Berkeley, so they know exactly what we all need and what we just merely want.
In this way, we can eliminate all uncertainties and provide security and happiness for all, just like the Constitution says, right?
And we do not have to worry about effects on “surplus populations”. Those mean Republicans would not have an argument anymore. And so, with this, happiness and prosperity forever was introduced into our land. Now, let’s all sing John Lennon’s “Imagine”.
SB 562 may be a good idea once it proponents actually figure out what the actual plan is. “Single payer” can mean many different things. Time to do actual policy work with details and analysis.
PGL:
what do you mean “what the actual plan is”.
“The Healthy California Program the bill envisions would cover all medical expenses without premiums, deductibles or copays. All state residents, including illegal immigrants, will be eligible. It would also ban insurers from covering anything already paid for by the legislation. Medicare and Medicaid enrollees, the privately insured, and those who get insurance through work—all would lose their existing coverage and become subject to the new state system.”
It is Paradise, PGL, it is Nirvana and Utopia combined – they teach that in Berkeley, and slowly, many other Economics departments around this great land.
All and everything will be covered, and we will all be happy.
And, as I said before, we should go for a single payer economy, where the government provides everything for us, cars, banking, air conditioners, education, insurance, everything.
And we go to work singing “Imagine”.
Manfred,
And, as I said before, we should go for a single payer economy, where the government provides everything for us, cars, banking, air conditioners, education, insurance, everything.
What you’re describing is not a single payer system. It’s called single provider. There’s a difference. If you want to join the conversation please learn the lingo. It’s kind of important.
Really Slugs. The elected arbiter of who joins the conversation, who, BTW, elected you to such position?
Well, well.
As far as I know and read in the press, the Canadian system is called single payer system, even though it is a single provider. The British health care system is called a single payer system, even though it is the government providing it (with private health insurance allowed, unlike Canada).
But, apparently, for you, semantics are more important than economics, and it shows.
Even taken at face value – people are only going to die if wealthy liberals choose not to address the problem with their own charitable giving.
We are constantly reminded of the affluence on blue states and the comparable poverty of red states. Why can’t successful blue state liberals solve this problem directly? Why does the problem require a federal solution?
Why is there an overabundance of money available to spend on special elections but no money to pay for these life and death concerns?
MINIMUM WAGE INCREASES, WAGES, AND LOW-WAGE EMPLOYMENT: EVIDENCE
FROM SEATTLE
This paper evaluates the wage, employment, and hours effects of the first and second phase-in of
the Seattle Minimum Wage Ordinance, which raised the minimum wage from $9.47 to $11 per
hour in 2015 and to $13 per hour in 2016. Using a variety of methods to analyze employment in
all sectors paying below a specified real hourly rate, we conclude that the second wage increase
to $13 reduced hours worked in low-wage jobs by around 9 percent, while hourly wages in such
jobs increased by around 3 percent. Consequently, total payroll fell for such jobs, implying that
the minimum wage ordinance lowered low-wage employees’ earnings by an average of $125 per
month in 2016. Evidence attributes more modest effects to the first wage increase. We estimate
an effect of zero when analyzing employment in the restaurant industry at all wage levels,
comparable to many prior studies.
……
We show that the impact of Seattle’s minimum wage increase on wage levels is much smaller than the statutory increase, reflecting the fact that most affected low-wage workers were already earning more than the statutory minimum at baseline. Our estimates imply, then, that conventionally calculated elasticities are substantially underestimated. Our preferred estimates suggest that the rise from $9.47 to $11 produced disemployment effects that approximately offset wage effects, with elasticity estimates around -1. The subsequent increase to as much as $13 yielded more substantial disemployment effects, with net elasticity estimates closer to -3.
There is no kink in the demand curve.
https://evans.uw.edu/sites/default/files/NBER%20Working%20Paper.pdf
Paying workers above a subsistence wage can raise productivity.
Steven Kopits,
This is a hot paper. I read it a few days ago. It’s a decent paper, but if you follow some of the econ sites you’ll find that quite a few economists have raised some pretty serious methodological problems with the study. The findings and the estimated elasticities are well outside anything that you’d find in most studies. In fact, they border on the implausible. Those elasticities look even more suspicious when you factor in the bizarre and hard-to-explain effects on workers making more than $19/hr.
-3 at $13. What a disaster. Even -1 at $11 is a failure.
What will the elasticity be at $15?
This is no surprise, but exactly what economic theory would predict. Why would anyone be surprised?
And just wait until we see the race, gender and age of those who lost their jobs.
By definition, raising pay will raise productivity by culling those who can’t generate their wage in value.
That doesn’t make a min wage a good idea.
People who cannot produce more value than a subsistence wage should be on disability.
And, it should be noted, when the country was beyond full employment in the late ’90s, bag ladies and guys sleeping in parks were hired. They were paid by temp agencies, e.g. $10 an hour. The temp agencies were paid, e.g. around $18 an hour (and were paying for workmans compensation insurance).
What’s subsistence value?
– Does a teenager living at home need more than subsistence value?
– Does an retired person living with family need more?
– Does a housewife looking for some extra cash need more?
– Does a Guatemalan who could earn $1 / hour in Guatemala or $11 / hour in the US need subsistence pay?
As for disability, I am guessing you will find it closely linked to the opioid crisis.
You cannot work full-time for less than $10 an hour in Seattle and be able to independently pay for your needs.
I suspect, you’ll need at least $12 an hour and very good benefits.
Of the 22M additional uninsured, how many are estimated to be people choosing to not buy insurance due to the removal of the mandate?
Dg – not allowed to ask those sorts of questions. Voluntarily choosing to not buy insurance is just another way the Republican health care bill kills people. (That 10,000 a year have been killed by Obamacare doesn’t matter either.) Get with the left-wing agenda here at Econobrowser.
How about the Supreme Court and that “MUSLIM” travel ban?
as i understand the new conservative bill, we will end up with fewer insured individuals and those that remain in the program will have progressively higher premiums, deductibles and max out of pocket expenditures than obamacare. but now we can either CHOOSE the more expensive health insurance, or we can CHOOSE to be uninsured. certainly provides an improvement over obamacare! again, we have been saved by the ideology of CHOICES.
What a trainwreck.
What problems were supposed to be addressed by this bill? The problem of high deductibles? The problem with high premiums? The problem of the “cliff” where one dollar more in income means you pay thousands more for insurance? The problem of health care inflation? McConnell’s bill does nothing to solve any of these pressing problems.
It’s a tax cut, pure and simple. A tax cut masquerading as a health care bill. It’s remarkable in its cynicism.
There was no health care problem to be addressed. The concern was always political. The Republicans made a promise, no matter whether they were capable of following through on that promise or not.
Better health care. Lower deductibles. Lower costs. Everybody covered.
Blah, blah, blah, for 84 months.
The true believers–unlike those actually paying attention to detail, including most medical professionals–bought in completely.
Bigger problem: there was no real thought re: creating better delivery of health care. Only appeasing the base and delivering on promises not to be kept. Current backslapping mentions deficit reduction, little about health care.
So what’s new?
There is a lot of rhetoric regarding both Obamacare and the new GOP proposals. What I would really like to see is a strict accounting of medical care before and after Obama care went into affect. How many people were denied medical care and died as a result before Obamacare and how many people were denied medical care and died as a result after Obamacare? Everybody has an opinion; I haven’t seen many facts.
+1