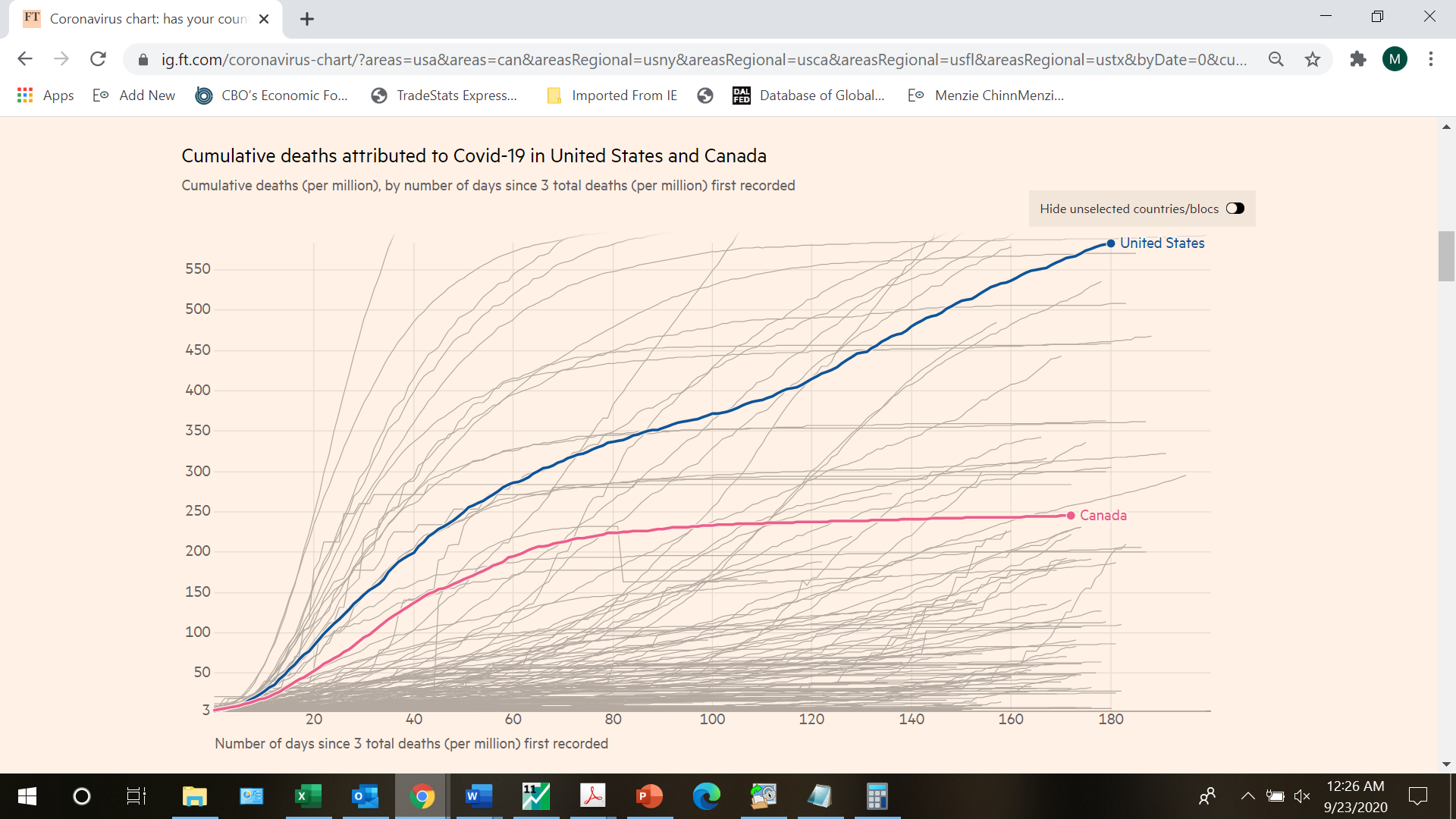
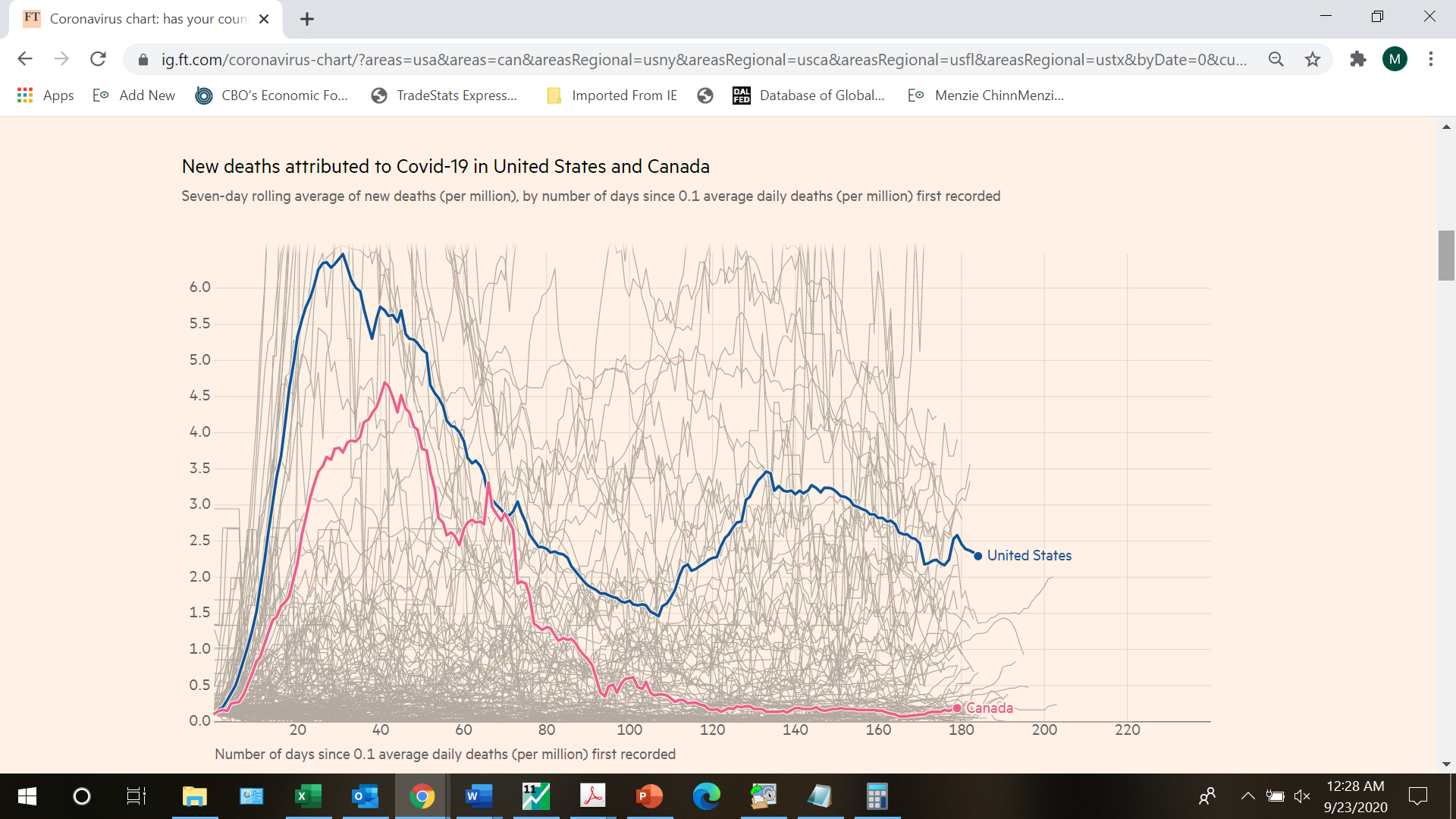
A reasonable person could ask why, if we’ve done such a superb job of managing the crisis in the US, we’ve done so poorly vis a vis Canada. From FT, today.
A reasonable person could ask why, if we’ve done such a superb job of managing the crisis in the US, we’ve done so poorly vis a vis Canada. From FT, today.
In the first two months, Canada’s numbers were rising almost as fast as our on a per capita basis but then they literally stopped rising while our daily death count has stayed high even on a per capita basis. But wait – you have turned the final corner and Trump grades his performance as an A+. These numbers suggest that this A+ is the most serious grade inflation ever.
So Bruce Hall is calling Kelly Anne Conway awaiting instructions of how to spin this.
It must be Canada’s socialist healthcare system. And the age old Canadian tradition, every time a Canadian NHL player scores a hat trick anyone over the age of 12 has to drink a pint of bleach.
Nah. It’s all those Emmys. They confer immunity.
Checkout the numbers for the county of Woodward Oklahoma people, my understanding is that for a county wide area, Woodward Oklahoma is now “leading” the nation, in Covid-19 cases per capita. Another “bragging point” for the illiterate “most red state” in the nation—Oklahoma. And as dumb Okies, we’re so proueeeeeeeeeeeewwwwwwd of that.
https://www.nytimes.com/interactive/2020/us/oklahoma-coronavirus-cases.html
The dust bowl exodus from Oklahoma improved the IQ of the California.
@dilbert dogbert
Debatable. But those were different times. If you had something analogous happening in current times, there would be no debate— California’s average IQ would drop.
SCIENTIFIC AMERICAN: COVID-19 CAN WRECK YOUR HEART, EVEN IF YOU HAVEN’T HAD ANY SYMPTOMS (8/31/20)
Re: Canada Vs the US, and why the marked difference in outcomes, to ask the question is to know the answer, to-wit, the Prime Minister of Canada accepts reality and deals with it, while Trump denies reality on a daily basis, at least in public.
The emerging evidence of a possible short-term to long-term health risk to people of all ages who have COVID-19 related myocarditis illustrates once again why Trump’s public statements (as opposed to what he privately told Bob Woodward) have been so wildly irresponsible and dangerous.
Myocarditis, an inflammation of the heart muscle, is usually caused by a viral infection. Myocarditis is currently the third leading cause of Sudden Death in children and young adults, and it most often affects otherwise healthy, young, athletic people.
For me, the bottom line is that, as the saying goes, actions speak louder than words, and the frantic pace of Coronavirus/Cardiac MRI testing of college and professional athletes speaks far louder than the whispers of some who are saying that you should move on—that there is nothing to see here.
Following are links to and excerpts from the 8/31/20 Scientific American article and to four subsequent articles, in chronological order, in MedPage Today, in Science Magazine and in The Atlantic.
The Atlantic article is somewhat more optimistic than the Scientific American article, with the others falling in between, in my opinion. The second MedPage article addresses the ongoing debate in medical circles regarding the use of Cardiac MRI (CMR) to detect myocarditis in persons who tested positive for the Coronavirus but who are otherwise asymptomatic for myocarditis. A multidisciplinary group is urging against general population screening for myocarditis.
Of course, there is a screamingly obvious double standard here, regarding the general population versus college and professional athletes, and one is reminded of the quote from the book “Animal Farm,” to-wit, “Some are more equal than others.”
Note that college (or at least college football players) and professional athletes are being routinely and repetitively tested for the Coronavirus, irrespective of symptoms, and then those who test positive are apparently getting repetitive CMR’s, to diagnose myocarditis. Athletes who test positive for myocarditis are usually sitting out the season.
In regard to Coronavirus testing, reportedly football players at larger Texas colleges are being tested three times a week and NFL players are being tested daily, except for game day.
Note that this daily to thrice weekly testing is being done on the favored few, even as the WSJ reports today that a lack of reagents is forcing health systems to limit who can get tested and end community testing programs.
The Red Sox’s 27-year old pitching ace, Eduardo Rodriguez, is a case in point. He had a symptomatic case of COVID-19, but after recovering, he said he felt fine, health-wise, i.e., he was asymptomatic for myocarditis. In his case, as one of the favored few, the myocarditis was picked up because of a precautionary series of CMR’s, and he is sitting out the season.
Obviously, colleges and professional sports teams have a financial interest to protect, in regard to protecting the health of their players, and they want to avoid the risk of competitive sports related sudden death.
But what about a 17-year old high school athletes or for that matter anyone of any age who experiences periodic periods of heavy exercise, e.g., a home Peloton machine?
Those of us not among the favored few could easily have had an asymptomatic case of COVID-19 and have a largely asymptomatic case of myocarditis—and everything is fine until they possibly experience serious arrhythmia or even sudden death, possibly while exercising.
A comment by “Dr JP,” following the 915/20 MedPage article advising against general population screening for myocarditis put it better than I can:
September 16, 2020
What if the first sign or symptom of cardiac problems is sudden cardiac death while running or spinning a month after Covid diagnosis with no or minimal symptoms?
This has nothing to do with “Choosing Wisely.” It has everything to do with protecting insurance companies.
The authors of the letter should have called for a national observational database for the registration of such patients tested in the community with long term follow up. I suspect most people who get tested would happily agree to be followed every 3-6 months. And why did they notify the Echo society? No echocardiograms either?
Soon the insurance industry will orchestrate “experts” demanding that state medical boards issue edits forbidding orders for CMR post Covid 19 unless ordered by some anointed academic.
Let me see if I understand the logic here: CMR testing post Covid is ok for high-priced revenue producing college athletes but not for ordinary people whose civic duty it is to suffer their myocardial damage silently and die or be disabled without testing.
And how are doctors on the front lines supposed to advise patients on their cardiac status post Covid? No symptoms, no problems? Just like in diagnosis? No symptoms, no disease?
What you don’t see won’t hurt you — until it does.
Dr JP
That is what concerns Ossama Samuel, associate chief of cardiology at Mount Sinai Beth Israel in New York, and he is studying a cluster of younger adults developing myocarditis, some of them a month or so after they had recovered from COVID-19.
Dr. Samuel called it extremely dangerous for athletes with myocarditis to play competitive sports for at least three to six months, because of the risk of serious arrhythmia or sudden death.
In any case, I don’t see why the potential health risk for a 17-year old high school student is any less than the potential health risk to a 27-year old MLB pitcher. The difference is that one is being constantly tested, while the other one is not.
Note that patients with myocarditis often experience symptoms like shortness of breath, chest pain, fever and fatigue, which obviously overlap with other diseases like COVID-19 itself and the flu, while others have no symptoms at all. A study of group of health care professionals who tested positive for myocarditis, following positive Coronavirus tests, found that the majority of them were asymptomatic for myocarditis.
Also, the other “Known unknown,” ad Donald Rumsfeld once said, is to what degree that post-COVID myocarditis represents a long-term health risk.
Note that Highland Park High School in Dallas, Texas last week had an illustrative case history of community spread of the Coronavirus among a group of young athletes. Eleven members of the varsity football team tested positive. As of this week the total Coronavirus positive test count for the high school is 24 students and two staff members. Note that this means that at least 26 families have been exposed, plus everyone that those family members exposed—and so on.
In any case, as Dr. Barber said in the final paragraph of the Scientific American article, in regard to those of us who are not being routinely tested, “And for the rest of us? Wear a mask, social distance, avoid large gatherings, and spend more time in the great outdoors. I would echo the advice of J.N.*, ‘Be careful. Just don’t get the virus in the beginning.’ As of today, it’s still the best defense we’ve got.”
*J.N. is a health care provider. Just 34 years old, he was diagnosed with COVID-induced myocarditis and severe heart failure. Doctors admitted him to the intensive care unit and placed him on a lifesaving intra-aortic balloon pump due to the very poor function of his heart. He spent two weeks in the hospital, has suffered recurrences since his discharge, and now says, “I’m very careful. I’m very concerned about the length of time I’ve been feeling sick, and if these symptoms are lifelong or will go away anytime soon.” J.N. said that everyday activities, like carrying his one-year-old daughter up a flight of stairs, leave him feeling winded and fatigued. He has been unable to work since March.
Scientific American: COVID-19 Can Wreck Your Heart, Even if You Haven’t Had Any Symptoms (8/31/20)
Carolyn Barber, M.D.
https://www.scientificamerican.com/article/covid-19-can-wreck-your-heart-even-if-you-havent-had-any-symptoms/?print=true
Carolyn Barber, M.D., has been an emergency department physician for 25 years. She is co-founder of the homeless work program Wheels of Change, and the author of many articles and a new book, Runaway Medicine: What You Don’t Know May Kill You.
Excerpt:
Samuel called it “extremely dangerous” for athletes diagnosed with myocarditis to play competitive sports for at least three to six months, because of the risk of serious arrhythmia or sudden death, and several athletes already have made the decision to heed those dire warnings. We’ll likely see more such decisions in the very near future, as each sport enters its peak season.
And for the rest of us? Wear a mask, social distance, avoid large gatherings, and spend more time in the great outdoors. I would echo the advice of J.N.: “Be careful. Just don’t get the virus in the beginning.” As of today, it’s still the best defense we’ve got.
MedPage Today: The Real Reason Post-COVID Myocarditis Is a Worry (9/8/20)
(Possible Long-Term Health Risk)
https://www.medpagetoday.com/infectiousdisease/covid19/88487
Excerpt:
Myocarditis is the top concern around COVID-19 for college athletics, due to the risk it poses for cardiac arrhythmia and sudden cardiac death. . . .
However, focusing on sports not only politicizes the findings but misses the point, Nagel argued in an interview with MedPage Today. . .
“We know that the presence of scar tissue, late enhancement by MRI, is prognostically relevant in almost any disease that has been looked at,” he said. “The same for inflammation.”
Even so, while that “will change their outcome statistically, again that doesn’t mean on an individual level,” Nagel said. “The person who has that doesn’t need to worry that they are now going to die sooner. But on a population level, if you have a million people with COVID and 22% of them develop more scar…there is a relevant risk that we’ll have a larger incidence of heart failure and chain of outcome in 10 years’ time.”
Science Magazine: As evidence builds that COVID-19 can damage the heart, doctors are racing to understand it (9/15/20)
https://www.sciencemag.org/news/2020/09/evidence-builds-covid-19-can-damage-heart-doctors-are-racing-understand-it
Excerpt:
Even if COVID-19 rarely causes serious myocarditis, one hypothesis is that mild cases could heighten the risk of heart disease years later. Scar tissue can form as myocarditis heals, and earlier work has shown residual cardiac inflammation portends worse heart health. As cardiologists, “We’re in the business of identifying asymptomatic risk factors,” such as hypertension, Mohiddin says. “It’s not difficult to imagine that in the future, clinical practitioners will ask a new patient, ‘Did you have COVID?’”
MedPage Today: Post-COVID Heart Scans Without Symptoms: Not a Good Idea (9/15/20)
https://www.medpagetoday.com/infectiousdisease/covid19/88633
Multidisciplinary group urges against general population screening.
The Atlantic: The Core Lesson of the COVID-19 Heart Debate (9/21/20)
https://www.theatlantic.com/health/archive/2020/09/covid-19-heart-pandemic-coronavirus-myocarditis/616420/
If athletes come down with clinical myocarditis—that is, with obvious signs of heart problems—they’re taken out of play for at least three months to let the infection run its course and to give the heart a chance to bounce back. The question now is: What to do about the people who have subclinical myocarditis after COVID-19, which presents with no symptoms and can be seen only on a medical scanner? Chokshi, the sports cardiologist, says the risk that these abnormalities will lead to heart failure “is very, very low,” but “the outcome is catastrophic.” The American College of Cardiology published guidance advising that all athletes who test positive for COVID-19 rest for at least two weeks, even if they show no symptoms.
Setting myocarditis aside, it still makes sense to stop players from spreading the virus to one another, especially when so many colleges are facing large outbreaks. “There are plenty of reasons to not play football independent of this issue,” Murthy says. “We already have plenty of evidence to take COVID-19 seriously.”
. . . Some claims about COVID-19’s effect on the heart may be overwrought, but that doesn’t mean the virus is harmless. Conversely, the claims that COVID-19 is equivalent to the flu are clearly wrong, but that doesn’t mean anything goes. The reality lies between this false dichotomy and is still grim, as evidenced by the sheer number of infections, deaths, and lingering disabilities. “It’s hard to find a balance,” says Rivera-Serrano. “It’s not an apocalyptic zombie virus that’s so different from everything else and can suddenly do all these things to the body. But you also don’t want to trivialize what is happening.”
The short version – this virus can kill you multiple ways or disable you if it doesn’t. And those who are favored get better care and better access to diagnosis.
When it comes to testing and treatment, insurance companies are aware that dead people are cheaper than sick people, so they would prefer that people died before diagnosis and treatment.
Did I miss anything?
Just that it’s another example of why Trump’s downplaying of the risk of COVID-19 is so dangerous, especially to young people, and what I find striking is that kids are engaging in team sport across the country that colleges and professional sports teams would not dream of letting their athletes engage in without repetitive Coronavirus testing—followed by Cardiac MRI’s for those who test positive.
And a “Rumsfeld Known Unknown” is to what extent that undiagnosed COVID-19 related myocarditis represents a potential long-term health threat, especially to those young people whom Trump inaccurately characterizes as almost totally immune to the Coronavirus. Note that a study of 26 Ohio State athletes who tested positive for the Coronavirus found some type of heart abnormality in a majority of them, 14 out of 26.
N YT: Covid-19 May Have a Hidden Impact on the Heart (9/23/20)
https://www.nytimes.com/2020/09/23/magazine/covid-myocarditis-heart-disease.html
Excerpt:
Last month, several college conferences, the Big Ten and the Pac 12 among them, postponed their sports seasons, including football, citing the risks posed to athletes by the coronavirus. A major factor in those decisions, according to some physicians, was the uncertain implications of a July paper in JAMA Cardiology . In this study of 100 people who had Covid-19, M.R.I.’s showed at least some signs of myocarditis in 60 of them, meaning they had inflammation in the heart muscle, which can weaken the organ and, on rare occasions, lead to sudden cardiac arrest. Another study, published this month in the same journal, looked at 26 Ohio State athletes who experienced Covid-19 with mild or no symptoms and detected evidence of possible myocarditis in five of them and lesser abnormalities in nine more. The condition poses a heightened risk to those whose physical activity puts stress on the heart: Even before the pandemic, myocarditis was a leading cause of death in young, otherwise healthy athletes.
It’s crucial to find out whether the coronavirus raises the risk of heart complications in people of all ages who are even mildly active. “Imagine if it turns out that 5 or 10 or 15 percent of asymptomatic or mild infections have clinical myocarditis on an M.R.I. — that would be unheard-of, in terms of how do we evaluate the safety for someone returning to exercise, regardless of their level of fitness,” says Jonathan Drezner, state director of the Center for Sports Cardiology at the University of Washington and a physician for the school’s sports teams, the Seattle Seahawks and others.
The problem is, no one knows how common myocarditis is in athletes or the general population — or, consequently, how likely it is to do harm. (Doctors typically advise those who get a diagnosis of myocarditis to wait three to six months before resuming activity.) Speaking of the abnormalities seen on the scans in the first JAMA study, Aaron Baggish, who directs the Cardiovascular Performance Program at Massachusetts General Hospital and is a team cardiologist for U.S. Soccer, U.S. Rowing and the New England Patriots, among other teams, says, “We simply have no idea whether they matter to any of these people.”
. . . It’s crucial to stop exercising and see a physician if you experience any symptoms of heart failure. People should be especially careful about resuming exercise after having Covid or another infection. But if you are not feeling sick, Baggish says, “maintaining a healthy exercise regimen is absolutely essential, because it actually increases the sensitivity of your immune system, so that if you do get infected, you’re likely to have a milder disease.” In weighing the risks of resuming team sports, he thinks, the primary concern should be “about controlling infection, both for athletes and for the communities that they live in, not the heart concerns.” If the prevalence of infection is above 1 or 2 percent, he says, “and you’re not doing any testing, then it’s almost certain that getting young people together is going to do more harm than good.”
September 22, 2020
Coronavirus
US
Cases ( 7,097,937)
Deaths ( 205,471)
India
Cases ( 5,640,496)
Deaths ( 90,021)
Mexico
Cases ( 700,580)
Deaths ( 73,697)
France
Cases ( 468,069)
Deaths ( 31,416)
UK
Cases ( 403,551)
Deaths ( 41,825)
Germany
Cases ( 277,176)
Deaths ( 9,491)
Canada
Cases ( 146,663)
Deaths ( 9,234)
China
Cases ( 85,297)
Deaths ( 4,634)
September 22, 2020
Coronavirus (Deaths per million)
US ( 620)
UK ( 615)
Mexico ( 570)
France ( 480)
Canada ( 244)
Germany ( 113)
India ( 65)
China ( 3)
Notice the ratios of deaths to coronavirus cases are 10.4%, 6.7% and 10.5% for the United Kingdom, France and Mexico respectively.
September 23, 2020
Coronavirus
Israel
Cases ( 200,041)
Deaths ( 1,316)
Deaths per million ( 143)
———————————–
July 4, 2020
Coronavirus
Israel
Cases ( 29,170)
Deaths ( 330)
Deaths per million ( 36)
https://twitter.com/paulkrugman/status/1305506522441699333
Paul Krugman @paulkrugman
I haven’t seen much reporting on Israel’s coronavirus disaster. But it shows how easily gains can dissipate if you get careless; and now they’re entering a second lockdown
https://pbs.twimg.com/media/Eh4XOAWWoAE0MRz?format=jpg&name=small
9:59 AM · Sep 14, 2020
Having apparently approached a containment of the coronavirus in June, the Israeli government incautiously opened schools and businesses, and the result has been a persistent community infection spread contributing to what are now 200,041 cases in the small country as compared to 85,307 in all through all of mainland China.
The simple explanation is ‘rugged individualism’ and the corollary is ‘don’t confuse me with science.’
Since you use FT as your authority, here is a different perspective they offer: https://www.ft.com/content/a2901ce8-5eb7-4633-b89c-cbdf5b386938
If we could only be like China… and not like New York or New Jersey. Also, note the section on “excess deaths”.
“If we could only be like China”:
This from the moron who advocates not social distancing. I guess you did not know China went for total lockdown. BTW – your obsession with blaming the victims of NY/NJ is not only gross but also dumb even for you. I guess you just refuse to recognize the fact that our region has dramatically reduced what was an early explosion whereas some parts of the nation are seeing rising daily death counts precisely because they followed your idiotic ideas whereas China did just the opposite of what you recommend.
I would say keep your childish stupidity coming as it amuses everyone in the same way a drunk clown amuses by constantly falling down. But I fear for your dog’s health as he can’t stop laughing at you either.
I realize FT provided a lot of data here. Apparently based on your stupid comment, you checked out NONE of this data. Permit me to point out one key paragraph:
”
Please use the sharing tools found via the share button at the top or side of articles. Copying articles to share with others is a breach of FT.com T&Cs and Copyright Policy. Email licensing@ft.com to buy additional rights. Subscribers may share up to 10 or 20 articles per month using the gift article service. More information can be found at https://www.ft.com/tour.
https://www.ft.com/content/a2901ce8-5eb7-4633-b89c-cbdf5b386938
“Europe’s average count of coronavirus-related deaths overtook Asia’s in early March, with Italy, Spain and the UK becoming the global hotspots. From mid-April the focus shifted to the US, where the number of deaths has remained consistently high, with the country currently accounting for nearly one in five global fatalities, although the focus of the epidemic has shifted from the northeast to southern and western states.”
In fact, NYC was the destination spot 6 months ago for a lot of infected Europeans which is why we got hit so hard early on. Of course Trump was too stupid to shut down flights from Europe. And you are too stupid to get this point even if everyone else does.
And notice the last part of this paragraph. NY/NJ has gotten this virus under control by being more like China whereas parts of the nation which have followed the Bruce Hall playbook are now the focus of the epicenter.
Come on Bruce – you do this routinely. Could you once in your pathetic trolling career actually READ the links you provide before you misrepresent what they say. JUST ONCE? DAMN!
Bruce Hall: Clicked on your link. That’s the page I go to to get to the source for by-country death rates…I’m not sure what you want me to read in the mass of text that makes me re-evaluate what I have written/posted.
Bruce clearly did not read this story.
Remember that the bulk of Canada’s population lives within 50 miles of the US
when thinking about the differences in their performance.
Good point but remember they had to good sense of not letting us Yanks cross the border.
Rand Paul in today’s coronavirus hearing spent his 5 minutes misrepresenting the evidence so he could attack Dr. Fauci’s recommendations for mitigation efforts. It was quite the show. Alas for the Senator, Dr. Fauci was able to give a few rebuttal words in basically noting how the Senator flat out lied.
I do hope someone puts up a tape of these 5 minutes and it was quite the show.
Rand Paul must have taken a pass on medical microbiology when he was in school. Of course, being an ophthalmologist doesn’t guarantee that he knows much about virus transmission
He never did complete his bs degree at baylor. And he is board certified by a board he created himself when he lost official board certification. He is the definition of a spoiled brat.
Here we go. Senator Rand Paul v. Dr. Fauci:
https://talkingpointsmemo.com/news/fauci-rand-paul-senate-hearing-coronavirus-lockdowns
Endure the absurdity of Rand Paul and the blow back he got from Dr. Fauci was just awesome.
Another “doctor”, in obstetrics, named Tom Coburn loved spreading ignorance on the Senate floor. He was also a Baptist deacon, not containing a single Christian bone in his body. On March 28 of this year God did us all “a solid”.
https://youtu.be/KVIDCSswc6E?t=508
Coburn died of prostate cancer, a genetic disease VERY common to men, and thought to be more treatable than in the past when men get it diagnosed early through testing.
Here’s 3+ minutes of it: https://www.cnn.com/videos/health/2020/09/23/senator-rand-paul-anthony-fauci-coronavirus-mitigation-efforts-nr-vpx.cnn
Thanks. I provided another story which has the entire clip.
When I listen to the utter BS from Rand Paul it strikes me as he has been reading the intellectual garbage from Bruce Hall. Or maybe Bruce is reflecting the intellectual garbage from Senator Paul. Sort of like the chicken or the egg.
Paul is like many Republicans, he “plays to the crowd” or “placates” the unwashed masses. He knows the differences between proper precautions and nonsense. He spouts nonsense because he’s well aware of the literacy levels of Kentuckians and what they like to hear. Ignorant people like their opinions repeated back to them~~~this is Paul’s modus operandi. You think a guy who went to Duke and smoked marijuana in college hasn’t partied and been good friends with many lefties?? He just tells the dumb guy at the carnival that the bearded lady “is real!!!!” and hands out darts that never quite hit the mark at a dollar per throw. Then goes in the backroom with the carnival operators and has 10 minutes of laughs on the latest yardbird he duped.
Do you remember Lindsay Graham’s little hussy fit for the Irish perv drunk up for Supreme Court?? You’ve seen better acting on “The Young and the Restless”. Democrats’ consistent biggest mistake is believing Republicans buy into their own bullet point cliches.
“Do you remember Lindsay Graham’s little hussy fit for the Irish perv drunk up for Supreme Court??
I like beer! I lift weights! Yep – a recipe for a rapist!
PGL, speaking of utterance intellectual garbage and scientific ignorance, from what I saw neither defined what they actually meant when talking about “herd immunity”. Following the science, you do believe we should follow the science don’t you? Herd Immunity Threshold (HIT) is defined as: ” Herd immunity, or community immunity, is when a large part of the population of an area is immune to a specific disease.” https://www.webmd.com/lung/what-is-herd-immunity#1
Immunity is not a binary condition but in reality is a conditional response ranging from full infection presenting all the symptoms and effects to infected and “asymptomatic”. Covid-19 has shown a high percentage of the populace falls into that latter category.
Accordingly estimating HIT is more complex than the simple formula because the estimate is based upon worse case scenarios assumptions. We’ve known early on that these assumptions are wrong. There are large number of asymptomatic cases, which indicates a level immunity already existed.
Several studies have estimated lower HIT. some as low as ~10% to 63%, but the latest peer reviewed study said: “Taking the effects of biological and social heterogeneity on COVID-19 transmissibility, the researchers calculate that the herd immunity threshold is likely somewhere between 20 and 30 percent of the population,” Proceedings of the National Academy of Sciences.” https://arxiv.org/abs/2008.08142
Without defining their terms which was more correct? I follow the latest science. Fauci appeared to not know about this study and Rand Paul did.
YOU OBVIOUSLY ALSO DO NOT KNOW ABOUT IT AND SEVERAL OTHERS.
CoRev: Useful to read and cite entire abstract. Last lines of abstract: “Our estimates suggest that the hardest-hit areas, such as NYC, are close to the heterogeneity-modified herd immunity threshold following the first wave of the epidemic. However, this type of immunity is fragile as it wanes over time if the pattern of social interactions changes substantially.”
You do know the difference between a peer-reviewed published article, and a “working paper” or “e-print”? At the top, in a red box…”Important: e-prints posted on arXiv are not peer-reviewed by arXiv; they should not be relied upon without context to guide clinical practice or health-related behavior and should not be reported in news media as established information without consulting multiple experts in the field.”
I have approved your comments w/o censoring in the past, but this really goes beyond the pale. Please stop wontonly spreading disinformation on such an important public health issue, either with good intentions or malevolently. Otherwise, I will ban you from Econbrowser.
Oh joy – someone who thinks Paul has the science correct. Come on CoRev – stop proving the obvious. You are a moron but we’ve known that for a long time.
Top line:
e-prints posted on arXiv are not peer-reviewed by arXiv; they should not be relied upon without context to guide clinical practice or health-related behavior and should not be reported in news media as established information without consulting multiple experts in the field.
Concluding line:
Our estimates suggest that the hardest-hit areas, such as NYC, are close to the heterogeneity-modified herd immunity threshold following the first wave of the epidemic. However, this type of immunity is fragile as it wanes over time if the pattern of social interactions changes substantially.
This was your link CoRev. I guess you just decided to omit key information. Try going back to what Fauci said at the end of his testimony as there is a relevant study that you either have not read or have chosen not to mention.
This isn’t the first time that CoRev has promoted something as “peer reviewed” research when it’s not. I don’t think CoRev understands what “peer reviewed” means in the context of academia. As best I can tell his idea of “peer reviewed” is when a couple of friends pass papers around and tell each other what a wonderful finding they’ve written. Then they have another round of beers at the watering hole. In any event, the paper he cited is recent, but is not “the latest” study on the subject.
“There are large number of asymptomatic cases, which indicates a level immunity already existed.”
hogwash. corev, you apparently do not understand what virus immunity means. just like in economics and science, you are wantonly ignorant of a topic and simply replace terms with your own interpretation of what they should mean. evidence of myocarditis in otherwise asymptomatic cases, for example, would suggest your understanding of immunity and asymptomatic is simply absurd. what it implies is that there are probably far fewer “asymptomatic” cases than you want to admit. you just choose to ignore some symptoms to come to your asymptomatic conclusion, covid corev.
“I don’t think CoRev understands what “peer reviewed” means in the context of academia. ”
corev has a habit of taking discipline specific terminology and redefining it in his “common sense” and “average joe” lexicon, and then arguing with you that your definition is simply wrong. unfortunately, he actually believes some of the crap he writes.
Menzie, not only is immunity not binary, Y/N, but a continuum of resistance. Instead of commenting on the “peer review” and the link? Considering the time to get a study peer reviewed, there are few that are a available. I do admit I relied on the source article for the peer review comment and reference link. If he’s wrong then so am I.
You are focusing on: ” However, this type of immunity is fragile as it wanes over time if the pattern of social interactions changes substantially.”” as if it is the signal of set events affecting immunity, even heterogeneity-modified herd immunity. The virus could mutate and or immunity lessen with times as it does with many cold viruses to create another wave of infections. Also, to think that the US populace is not intelligent to follow the social distancing guidance is a logical stretch. Those in the threatened cohort are assuredly following them. the young are doing what they always do until they or their friends too get bitten by Covid.
If this were the only study with similar results it might be reasonable to ignore it, but it isn’t. The science on Covid is moving and changing very fast. Your article re: CDC testing guidelines changes is an example. The latest admission from CDC is that the testing supplies are again in short supply, and local entities are self limiting their tests accordingly.
Sounds suspiciously like the mask issue all over again, no, yes use masks/do PCR tests. All because of supply shortages. Not Trump’s direction.
For some reason there is a belief that there is only one scientific interpretations. Your own experience shows that not to be true. When you say: “but this really goes beyond the pale.” implies there is only one interpretation OR WORSE THE COVID-19 SCIENCE IS SETTLED. Do you really believe the science surrounding Covid-19 is settled and there is nothing new being written to be eventually peer reviewed?
CoRev: Please, please, please, for the love of g** cite what you claim in your statement “If this were the only study with similar results it might be reasonable to ignore it, but it isn’t.”
AFAIK none are peer reviewed. There is a wealth of contradictory studies where only time and more research will prove which are more valid. As I implied earlier that is not uncommon with such a fast moving, changing science. Consensus does not prove valid science.
Herd immunity and social heterogeneity.
https://science.sciencemag.org/content/369/6505/846.full
https://www.medrxiv.org/content/10.1101/2020.07.23.20160762v1?versioned=true
https://www.medrxiv.org/content/10.1101/2020.04.27.20081893v3
https://www.sciencedaily.com/releases/2020/06/200623111329.htm
https://www.medrxiv.org/content/10.1101/2020.05.19.20104596v1.full.pdf
To speculate why there is a high asymptomatic rate or increased resistance to the Covid-19 virus.
https://science.sciencemag.org/content/early/2020/08/04/science.abd3871
“Thus, variegated T cell memory to coronaviruses that cause the common cold may underlie at least some of the extensive heterogeneity observed in COVID-19 disease.”
https://www.sciencedirect.com/science/article/pii/S0092867420306103
“Importantly, we detected SARS-CoV-2-reactive CD4+ T cells in ∼40%–60% of unexposed individuals, suggesting cross-reactive T cell recognition between circulating “common cold” coronaviruses and SARS-CoV-2.”
“The latest admission from CDC is that the testing supplies are again in short supply, and local entities are self limiting their tests accordingly.”
corev, you confuse science with logistics. they are not the same. when mask use or testing is reduced by logistics, that does not mean the science says we no longer need them. idiot.
“Immunity is not a binary condition”
it is more binary than you want to admit. the response is a continuum, but you either get an immune response, or not, based upon your exposure to a virus. this goes back to your silly comments trying to link asymptomatic cases to herd immunity. asymptomatic people are not immune, they have the virus. and the virus can spread. and some of those who then catch it are not asymptomatic, and will die. again, corev, you have a misunderstanding of the difference between somebody who is immune to the virus, and someone who is asymptomatic but a carrier of the virus. stop confusing the two cases.
CoRev Why do you continue to post observational and exploratory studies as though they are useful for public policy purposes? Most of the studies you posted present hypotheses that invite additional research. That’s it. That’s all they do. Those studies are neither definitive nor peer-reviewed. Some of the speculations may or may not pan out, but we won’t know that for years to come. Also, notice that many of the studies that speculate about a relatively low herd immunity level were written several months ago. That’s important because those studies would have a hard time explaining the most recent spikes in cases across Europe in regions that had infectivity levels far in excess of what 20% levels of herd immunity would predict; e.g., Paris, Lombardy, Spain and the UK. At a minimum that fact ought to make you pause before putting too much weight on any theory that predicts low levels of herd immunity. And have you given any thought as to what a persistent heterogeneity HIT implies with respect to public policy choices? Think it over.
Baffled, your comment : “the response is a continuum” confirms what I said.
For the rest of your comment, you read more into what was written than what was there. As for your comment: “you have a misunderstanding of the difference between somebody who is immune to the virus, and someone who is asymptomatic but a carrier of the virus. stop confusing the two cases.” I refer you again: “the response is a continuum”. You and much of the literature are confusing presymptomatic to asymptomatic. I don’t doubt some level of infections are caused by asymptomatic individuals, and also believe they are relatively mild cases. I also believe more infections are caused by those presymptomatic individuals.
“… Asymptomatic residents who tested positive were reassessed 7 days later. … Of these 48 residents, 27 (56%) were asymptomatic at the time of testing; 24 subsequently developed symptoms (median time to onset, 4 days). ” https://pubmed.ncbi.nlm.nih.gov/32329971/
There are other studies showing that those individuals with more severe symptoms also have heavier viral loads and heavier shed rates making them more likely to infect others. (I’ll let you do your own research.) It would be rare to find high viral loads in asymptomatic individuals.
“It would be rare to find high viral loads in asymptomatic individuals.”
corev, since you could not be bothered with some basic research. asymptomatic individuals are a PROBLEM.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7291769/
from the paper, “The viral load detected in nasopharyngeal swabs of asymptomatic carriers is relatively high, with a great potential for transmission. ” please read the paper completely.
“You and much of the literature are confusing presymptomatic to asymptomatic. I don’t doubt some level of infections are caused by asymptomatic individuals, and also believe they are relatively mild cases. I also believe more infections are caused by those presymptomatic individuals.”
let me get this right. from the guy who did not graduate with a stem degree (and may not have graduated from college at all), you have the insight to say the medical doctors writing about covid today are simply confused by the presymptomatic and asymptomatic characterization. perhaps the good dr corev should offer his world class medical courses to the current uneducated doctors of the world. perhaps you can do that in between your world class lectures on global climate, of which you also seem to think you know more than the experts. you are too stoooopid to understand the magnitude of your ignorance, corev.
2slugs, in fast changing science environment WITH LIVES ON THE LINE non-peered reviewed studies are often all that’s available. Only in your world does waiting fro full peer review not cost lives. Nor in your world does getting new research out to the world’s scientists ASAP not make sense. For some strange TDS-driven reason you think this is bad: “Most of the studies you posted present hypotheses that invite additional research.”
Baffled, wow! Contradictory study results. How can that be science if there is no consensus?
CoRev in fast changing science environment WITH LIVES ON THE LINE non-peered reviewed studies are often all that’s available. Only in your world does waiting fro full peer review not cost lives.
Sorry, but this makes absolutely no sense. Even if we suppose that those studies are correct, the implied policy choices from an assumed 20% HIT do not reduce deaths. The authors of the study make no such claim. I suspect that you didn’t read their paper. And following CDC guidance does not increase the number of deaths. Even if those studies are right about a 20% HIT, all that means is that assuming a higher HIT carries greater than necessary inconvenience costs like wearing a mask and social distancing. Following CDC’s guidance does not increase the number of deaths relative that we would see even if those 20% HIT studies turn out to be correct. This isn’t a case of balancing two approaches in which a new and unproven theory promises lower deaths. OTOH the reverse is not true. The risks of assuming a 20% HIT are highly asymmetrical. Your comment is a perfect example of what I mean when I talk about your poor analytical skills. In any event, real world developments in Europe strongly argue against the theory that HIT can be achieved with 20%. If that theory were true, then we should not be observing the big spike in cases that we’ve been seeing over the last week.
2slugs, what are you talking about now? 20% HIT less/more deaths? Are you on crack? Only you have been talking about changing policy and deaths. Don’t you remember asking this? “And have you given any thought as to what a persistent heterogeneity HIT implies with respect to public policy choices? Think it over.” Why such an inane question?
You seem to enjoy circular arguments with yourself.
“Baffled, wow! Contradictory study results. How can that be science if there is no consensus?”
no corev. the consensus is what i stated. asymptomatic spreads the virus. that is what the science says today. you use words like “i believe” and “i doubt” quite often, and seem to confuse your words with the facts. you are simply an idiot.
CoRev Only you have been talking about changing policy and deaths.
Excuse me for absent mindedly assuming you have an IQ above room temperature. I asked you what was your purpose in posting so many unproven studies. You replied that when lives were at stake you often don’t have the luxury of waiting for complete analyses and evaluations. That’s fair enough and I don’t disagree. But that implies that those unproven studies somehow promise new treatments or policies that would lower death rates relative to the status quo. The studies you linked to made no such claim. Whether the HIT is 20% or 60% makes absolutely no difference to whether or not public policy should encourage social distancing or the wearing of masks. In fact, your own link made that point quite explicitly. Suppose policymakers took seriously the claim that HIT could be achieved with a 20%. What kinds of policies would that imply? Well, it would mean less need for vaccines and PPE. That wouldn’t be a problem if the true HIT was in fact 20%, but it would be a catastrophe if the theory was wrong and the true HIT was 60%. OTOH, in the reverse case in which the theory is right and the true HIT is 20% but policymakers assume 60%, there would be no more deaths than under the alternative hypothesis but there would be the extra cost of producing more vaccines and PPE. The point is that the consequences of being wrong are asymmetric. In terms of public policy there is no value in assuming an unproven theory of 20% HIT. It might be of interest to epidemiologists and virologists, but you and I are neither.
All of this ought to have been blindingly obvious, but for some reason you don’t seem to get it. Poor reasoning skills? Old age? Or those physical changes in the brain that neurologists have identified with so many older, conservative men?
Baffled, there you go again arguing something while missing the sarcasm of consensus science. I guess in your world there can never, never, ever be a scientific breakthrough by an individual or minority of scientists. SCIENCE ONLY OCCURS BY THE MAJORITY (CONSENSUS)!
Wow, Baffled, miss many points? 1st, who said that asymptomatic Corona individuals can not, spread the virus? Not I and not my references.
I guess you also missed the sarcasm associated with consensus science. In your world science can only be done or accepted by the majority of scientists (consensus). In your world there can be NO SCIENTIFIC BREAKTHROUGHS BY INDIVIDUALS OR SMALL NUMBER OF SCIENTISTS ONLY THE MAJORITY?
2slugs, I laughed so hard my computer is now coffee covered.
“CoRev Only you have been talking about changing policy and deaths.
(ad hominem deleted) You replied that when lives were at stake you often don’t have the luxury of waiting for complete analyses and evaluations. That’s fair enough and I don’t disagree. But that implies that those unproven studies somehow promise new treatments or policies that would lower death rates relative to the status quo. The studies you linked to made no such claim….”
NOR HAVE I. ONLY YOU REPEATEDLY!
(The remainder of the comment continues your argument with yourself and more ad hominems.)
You still fail to understand what the HIT actually means.
“ It would be rare to find high viral loads in asymptomatic individuals.”
Corev, You are arguing that asymptomatic is not a problem. The studies, including the one i gave you, indicate your statement is false. Your inability to accept this is why you are an idiot.
CoRev
The studies you linked to made no such claim….”
NOR HAVE I. ONLY YOU REPEATEDLY!
Okay, that’s fine. And since you have a reputation for “pulling a CoRev”, let’s nail this down. Is it fair to say that you are only posting studies on heterogeneous HIT out of general interest and that you are not suggesting any concrete policy decisions follow from those studies? So you still think policymakers should proceed as though the true HIT is 60% and not 22%, right? That means you disagree with Sen. Rand Paul who doesn’t support the CDC’s social distancing and mask wearing guidelines. Just want to get you on the record.
Alas Dr. Birx may retire from the COVID19 task force as she is being sidelined by liars like Scott Atlas:
https://talkingpointsmemo.com/news/stanford-medical-faculty-letter-scott-atlas-trump-covid
Stanford Med Faculty Rips Trump’s New Favorite COVID Doc: Peddling ‘Falsehoods’
A group of 78 researchers and doctors from Stanford Medical School issued a letter on Wednesday that rebuked Dr. Scott Atlas, who President Trump appointed to the White House coronavirus task force last month, for peddling “falsehoods and misrepresentations of science.” Atlas —a neuroradiologist who is not an epidemiologist and has no significant experience with treating infectious diseases — was a regular fixture on Fox News prior to joining the White House coronavirus task force last month. Atlas often bolstered Trump’s public downplaying of COVID-19 by dismissing the need to wear masks to reduce the spread of the novel coronavirus, advocating for in-person instruction to resume at schools amid surging COVID-19 cases nationwide and asserting that it was “very important” that herd immunity develop even before a vaccine was ready. In a “Dear Colleagues” letter issued on Wednesday, the Stanford experts wrote that they have a “moral and ethical responsibility” to dispute Atlas’ unfounded claims on COVID-19, which they described as “opinions and statements (that) run counter to established science” and “undermine public health authorities and the credible science that guides effective public health policy.” Although the letter did not specifically cite Atlas’ past comments, the Stanford experts included a list based on a “preponderance of data” that disproved Atlas’ controversial assertions — which include denouncing the use of natural “herd immunity” as “not a safe public health strategy” that there can have “serious short-term and long-term consequences” for children and young people who contract COVID-19. The Stanford experts concluded their letter by warning against the “failure to follow the science – or deliberately misrepresenting the science,” which they wrote “will lead to immense avoidable harm.” The White House did not immediately respond to TPM’s request for comment.
That Stanford Letter:
https://www.pids.org/resources/covid-19/822-open-letter-from-stanford-university-regarding-dr-scott-atlas.html
Open Letter from Stanford University regarding Dr. Scott Atlas
September 9, 2020
Dear Colleagues,
As infectious diseases physicians and researchers, microbiologist and immunologists, epidemiologists and health policy leaders, we stand united in efforts to develop and promote science-based solutions that advance human health and prevent suffering from the coronavirus pandemic. In this pursuit, we share a commitment to a basic principle derived from the Hippocratic Oath: Primum Non Nocere (First, Do No Harm).
To prevent harm to the public’s health, we also have both a moral and an ethical responsibility to call attention to the falsehoods and misrepresentations of science recently fostered by Dr. Scott Atlas, a former Stanford Medical School colleague and current senior fellow at the Hoover Institute at Stanford University. Many of his opinions and statements run counter to established science and, by doing so, undermine public-health authorities and the credible science that guides effective public health policy. The preponderance of data, accrued from around the world, currently supports each of the following statements:
The use of face masks, social distancing, handwashing and hygiene have been shown to substantially reduce the spread of Covid-19. Crowded indoor spaces are settings that significantly increase the risk of community spread of SARS-CoV-2.
Transmission of SARS-CoV-2 frequently occurs from asymptomatic people, including children and young adults, to family members and others. Therefore, testing asymptomatic individuals, especially those with probable Covid-19 exposure is important to break the chain of ongoing transmission.
Children of all ages can be infected with SARS-CoV-2. While infection is less common in children than in adults, serious short-term and long-term consequences of Covid-19 are increasingly described in children and young people.
The pandemic will be controlled when a large proportion of a population has developed immunity (referred to as herd immunity) and that the safest path to herd immunity is through deployment of rigorously evaluated, effective vaccines that have been approved by regulatory agencies.
In contrast, encouraging herd immunity through unchecked community transmission is not a safe public health strategy. In fact, this approach would do the opposite, causing a significant increase in preventable cases, suffering and deaths, especially among vulnerable populations, such as older individuals and essential workers.
Commitment to science-based decision-making is a fundamental obligation of public health policy. The rates of SARS-CoV-2 infection in the US, with consequent morbidity and mortality, are among the highest in the world. The policy response to this pandemic must reinforce the science, including that evidence-based prevention and the safe development, testing and delivery of efficacious therapies and preventive measures, including vaccines, represent the safest path forward. Failure to follow the science — or deliberately misrepresenting the science – will lead to immense avoidable harm.
We believe that social and economic activity can reopen safely, if we follow policies that are consistent with science. In fact, the countries that have reopened businesses and schools safely are those that have implemented the science-based strategies outlined above.
As Stanford faculty with expertise in infectious diseases, epidemiology and health policy, our signatures support this statement with the hope that our voices affirm scientific, medical and public health approaches that promote the safety of our communities and nation.
Stanford? OK, but we’ll wait for the definitive statement on this from the medical faculty at Northeast Texas State . Both men are renowned experts in their fields ( equine and canine disease) and should be able to counter the know-it-all left coasters quite nicely.
Israel recorded 9,762 coronavirus cases this today. The health and resultant economic consequences of an incautious opening of schools and businesses have been devastating:
September 23, 2020
Coronavirus
Israel
Cases ( 203,136)
Deaths ( 1,316)
Deaths per million ( 143)
@ ltr
I’m so glad you’re on this blog ltr, you give me added motivation to post more about what Beijing does to its own people everyday:
https://www.nytimes.com/2020/09/24/world/asia/china-muslims-xinjiang-detention.html?action=click&auth=login-email&login=email&module=News&pgtype=Homepage
How is Huang Kunming doing lately ltr ??? If he hired you he needs to have his A$$ fired immediately.
September 23, 2020
Coronavirus
Spain
Cases ( 693,556)
Deaths ( 31,034)
Deaths per million ( 664)
Portugal
Cases ( 70,465)
Deaths ( 1,928)
Deaths per million ( 189)
[ The difference proper public health policy makes is remarkable and scary. ]
September 23, 2020
Coronavirus
Dominican Republic
Cases ( 109,737)
Deaths ( 2,074)
Deaths per million ( 191)
Cuba
Cases ( 5,270)
Deaths ( 118)
Deaths per million ( 10)
[ Dominican Republic has had the fastest growth in per capita GDP in all the Americas since 1971. Cuba has been beset by fierce economic sanctions all these years, sanctions that have been added to by this administration and in this pandemic. Nonetheless, look to the health characteristics of Dominican Republic and Cuba and from infant mortality to life expectancy to faring through the pandemic Cuba is distinguished. ]
Oklahoma had 8 deaths today. Hospitalizations is the number most closely associated with an anticipated rate of deaths, the number jumped over 100 on Tuesday, then dropped 16 on Wednesday, and when a state health official was asked about the over 100 increase in hospitalizations he said “several hospitals didn’t report numbers over the weekend”. So every weekend we get the reports of only 1-2 deaths on a Sunday and state officials all jump up and down and do cartwheels like we have it beat and then when the number jacks up again they say “well several hospitals didn’t report”. It seems like Governor Stitt has taken a page out of the orange creature’s book and is bullying state health officials (they’ve already gone through two different head epidemiologists and are now working on their third). All you have to do is look at the numbers for hospitalizations and the 7-day moving average on deaths and you know they are all full of crap–and we are probably about to hit another “wave” in both cases and deaths. Of course whenever the Governor has a press conference or what some media call in slang “a presser” we never get to see those graphs. Observe the graph Oklahoma’s Governor Kevin Stitt likes to play “hide and seek” with, with his voters.
https://twitter.com/pmonies/status/1308800355979927552/photo/3
It never seems to jump to the graph I want it to jump directly to, it goes to the tweet—the hospitalizations graph is the orange colored bar graph in the lower left quadrant of the first tweet you see after the link jump. Deaths graph is the medium shade of blue bar graph in the upper right quadrant, with an accompanying orange line that depicts the 7-day moving average. You can see that number has remained relatively steady since the increase in late July, but is giving some indications it may hit the late August peak again in the very near future.
About Israel, which distressingly recorded 11,316 new coronavirus cases today, the failure to contain the spread of infections reflects a structural healthcare problem that was understood even as Israel incautiously opened schools and business. Israel has had a medical laboratory or testing problem for quite a while, so that in opening schools and businesses there was a lack of testing and analysis. This problem was understood from the time of the opening, written about in China, but correcting such a problem is costly in resources and under the circumstances slow to correct.
The patterns to be found in looking to the pandemic are repeatedly reflections of domestic public health or healthcare development.
Anthony Fauci Basically Calls Rand Paul a Shameless Moron to His Face
The COVID-19 expert was having none of the lawmaker’s bullshit on Wednesday.
https://www.vanityfair.com/news/2020/09/anthony-fauci-rand-paul-coronavirus
I watched this show live yesterday. It seems Senator Paul managed to capture the BS from Bruce Hall, CoRev, and Sammy in his 5 minutes of shame.
September 24, 2020
Coronavirus
Israel
Cases ( 209,635)
Deaths ( 1,376)
Deaths per million ( 150)
———————————–
July 4, 2020
Coronavirus
Israel
Cases ( 29,170)
Deaths ( 330)
Deaths per million ( 36)
September 24, 2020
Coronavirus
Spain
Cases ( 704,209)
Deaths ( 31,118)
Deaths per million ( 665)
Portugal
Cases ( 71,156)
Deaths ( 1,931)
Deaths per million ( 190)
the difference is the Canadian Healthcare system is better and more efficient. the Canadians spend 12 % of GDP and the US spends 18 % of GDP before the crisis. the US system is riddled with waste. Overpriced drugs, that are given huge monopolies in terms of patents. Dr’s that are protected from free market competion. the AMA says who can become a Dr. there are 1600 insurance companies with their multimillion CEO’s pay packages and vice-presidents. In fact, the Medicare system in the US only charges 3% of administrative expenses.
whereas the Canadian system has a …single payment. the federal govt.
Communist!!!!!
ad hominin attack or sarcasm?
Indictment of those who believe health care should operate as a capitalist free market. Works well while sitting in an emergency room surfing the net for a cheaper surgeon to remove your spleen.
You do know the U.S. reports lower health outcomes that other Industrialized countries. For example, Houston has the highest mortality rate for women who are giving birth so the lesson is do not get sick in Texas! that capitalist paradise.
i think we are in agreement here, ooe, that free markets do not operate well in healthcare.
“For example, Houston has the highest mortality rate for women who are giving birth so the lesson is do not get sick in Texas! ”
i will point out that this is a bit misleading. houston population may have a high mortality rate associated with birth, but it probably has more to do with the fact the texas medical center is located in houston, and hosts several of the largest and best childrens and women’s hospitals in the nation. these hospitals typically do not handle routine care, but they handle the severe birth cases throughout texas and the south. a big part of the mortality rate is because they take in cases from outside of houston that many hospitals cannot handle. these can still have poor outcomes, and this helps drive up the houston mortality rate.
CoRev bombards us with other links he does not understand. First link is some mathematical model which is cool but equations are not evidence. In the header of his 2nd link we read:
“This article is a preprint and has not been peer-reviewed [what does this mean?]. It reports new medical research that has yet to be evaluated and so should not be used to guide clinical practice.”
What does not being peer-reviewed mean? CoRev clearly does not know. This is better than The Onion!
BTW CoRev – click on that passage and it will explain to you the importance of being peer reviewed or not.
I swear Bruce Hall is got some real competition for linking to articles he has not bothered to read!
There seems to be a lot of discomfort and misunderstanding of Herd Immunity Threshold (HIT). Hopefully this article will shed some light.
https://www.quantamagazine.org/the-tricky-math-of-covid-19-herd-immunity-20200630/
Many recent studies talk about the populace heterogeneity to Corona-19. This is what it means:
“Epidemiologists refer to these variations as the “heterogeneity of susceptibility,” meaning the differences that cause some people to be more or less likely to get infected.”
and
“Usually, researchers only think about herd immunity in the context of vaccine campaigns, many of which assume that everyone is equally likely to contract and spread a disease….” That’s the homogeneous view. ” But in a naturally spreading infection, that’s not necessarily the case. Differences in social behaviors lead some people to have more exposure to a disease than others. Biological differences/b> also play a role in how likely people are to get infected.” CDC estimates that as high as 40% of Covid-19 cases are asymptomatic.
Also: “However, in an ongoing pandemic with no guarantee that a vaccine will be available anytime soon, the heterogeneity of susceptibility has real implications for the disease’s herd immunity threshold.
In some cases it will make the threshold higher. This could be true in places like nursing homes, where the average person might be more susceptible to COVID-19 than the average person in the broader population.
But on a larger scale, heterogeneity typically lowers the herd immunity threshold. ” And
“Many experts, however, consider these new studies — not all of which have been peer-reviewed yet — to be unreliable.”
Perhaps the biggest misunderstanding is around the term “threshold”. Once HIT is achieved: “At that point, the virus will still spread, but at a decelerating rate until it stops completely. Just as a car doesn’t come to a stop the moment you take your foot off the gas, the virus won’t vanish the moment herd immunity is reached. : ”
Your desperate over reactions to a still to be defined inflection point in the infection rate variable is hilarious. Fauci reacted in the same manner to the same inflection point in the infection rate variable. It is highly unlikely that Fauci is more correct than Rand Paul?
Rand Paul to: “Dr. Fauci – this article in Science proposes that heterogeneity of human populations allows for non-random transmission where immunity concentrates in younger less vulnerable members of the population. Therefor herd immunity may occur at less than 2/3rds”
“FAUCI to Sen. Paul: “You are not listening … If you believe that 22% is ‘herd immunity’, I believe you’re alone in that.”
Nope! Not alone.
Let the fight begin around the veracity of any number associated with HIT.
Sorry about the highlight typo.
CoRev: 22% – near enough alone, from my reading of the article you cited. You should read up on optimal-decisionmaking under uncertainty. Pulling back on responsiveness is not the way to go; reacting a bit more than based on point estimate is. So, the point is: Don’t engage in wishful thinking when deciding on response.
I shudder to think that someone like CoRev would ever find himself in a position of responsibility when evaluating decision/risk models. The idea of CoRev as a decision maker in military scenarios with asymmetric risks and extreme uncertainty is downright frightening.
CoRev has of late been busy saying his herd immunity “evidence” is not a recommendation to skip social distancing / mask wearing.
I guess CoRev did not listen carefully to that crap from Senator Paul as that is exactly what he was recommending. It is also what Trump at times recommends as well as people like Bruce Hall.
Now CoRev may think he is defending these fools but any supposed evidence of that unicorn known as herd immunity is a far cry from the policy agenda of these clowns. If CoRev does not get this, maybe he in over his head more than we could ever imagined.
Menzie, a strawman argument??? “Pulling back on responsiveness is not the way to go;…” Other than 2slugs, I know of no one who has suggested that. This seems to be an incomplete or unsupported thought: ” reacting a bit more than based on point estimate is.”
This discussion started with Fauci’s claim that Rand Paul was alone in his thinking. For which i cited what I thought was the study to which he referred, and said there were others. You then asked for cites, which I provided.
2slugs is the only one talking about the policy implications of a low HIT. Not I, and AFAIK nor are my references.
I don’t know how you can reach this conclusion: “CoRev: 22% – near enough alone, from my reading of the article you cited.” except that you ignored the multiple references provided.
I therefore take your advice: “So, the point is: Don’t engage in wishful thinking when deciding on response.” with a heavy dose of salt.
“This discussion started with Fauci’s claim that Rand Paul was alone in his thinking.”
I see – you have stumbled onto a cult of insane scientists. Safety in numbers or One Flew Over the Cuckoo’s Nest?
CoRev Apparently all of this was news to you. I assure you, it wasn’t news to most of us. All of us are more than aware of the difference between heterogeneity HIT and HIT assuming an homogenous population. The system of standard linear ODE equations used to model infections explicitly assumes homogeneity across the susceptible population. We all know this.
Again, what are the practical policy differences between a 22% heterogeneous HIT and a 60% homogeneous HIT? If African-American and Hispanic populations are at a higher risk than white Americans, does that mean we should just accept higher infection and mortality rates among the more vulnerable populations? Sen. Paul is an ophthalmologist and has no expertise whatsoever in epidemiology. He knows just enough to be dangerous because rubes like you are easily conned.
Let the fight begin around the veracity of any number associated with HIT.
Fine, but let the “fight” be between qualified experts and not blog posters who can’t even follow the math in a short paper that you yourself linked to:
https://arxiv.org/pdf/2008.08142.pdf
In any event, Sen. Rand Paul and Dr. Fauci were not talking about heterogeneous HIT; they were talking about various studies that have been looking at cross-reactivity immunity with other coronaviruses. But I will grant you that Sen. Paul did seem to conflate the 22% heterogeneous HIT number with cross-reactivity studies, but in his comment to Dr. Fauci Sen. Paul did explicitly ask Dr. Fauci if he was aware of the cross-reactivity studies. Sen. Paul just demonstrated the confusion in his own mind between the two studies and somehow got them all jumbled. In any event, Dr. Fauci replied that was aware of the cross-reactivity studies and was also aware of a very recent study that disputed some of the earlier studies.
“The system of standard linear ODE equations used to model infections explicitly assumes homogeneity across the susceptible population. We all know this.” AND THAT COULD NEVER BE THE WRONG ASSUMPTION? ESPECIALLY WHEN ESTIMATING/ANALYZING HIT WITHOUT A VACCINE????
2slugs, more straw for your man? “Again, what are the practical policy differences between a 22% heterogeneous HIT and a 60% homogeneous HIT?” Why do you continue to beat the dead straw horse? Why do you even think there would be any difference? I have never mentioned or recommended any policy differences. Perhaps you don’t understand asking such a general question adds no value.
I don’t know how you limited the Paul/Fauci discussion to: ” they were talking about various studies that have been looking at cross-reactivity immunity with other coronaviruses.” The only study cited we’ve been discussing, and it surely is not limited to that. Maybe this is what Menzie meant in wishful thinking?
Another big scientific whoop: “…Dr. Fauci replied that was aware of the cross-reactivity studies and was also aware of a very recent study that disputed some of the earlier studies.” Contradictory studies???? Wow! That can’t be modern science.
You’ve used some of the worst possible argument formats without discussing the contents of my comments. At least you have admitted that the HIT rate is up for discussion.
“At least you have admitted that the HIT rate is up for discussion.”
This is like saying the gold standard is up for discussion re monetary policy AND annually balancing the budget is a form of fiscal policy.
Fine discuss crack pot ideas but making general policy based on crack pot ideas is never a good idea. Oh wait – you protest that you are not recommending herd immunity as a policy but the crack pots you insist on defending are.
CoRev Why do you continue to beat the dead straw horse? Why do you even think there would be any difference?
Why can’t you answer a simply yes/no question in a straightforward way? Ever wonder why you get banned from so many websites? Maybe it’s because you argue in bad faith. If you don’t believe there would be any policy differences between a 22% HIT and a 60% HIT, then you are arguing against Sen. Rand Paul, because Sen. Paul was saying NY is already at herd immunity and there shouldn’t be anymore restrictions. If you want to disagree with Sen. Paul, then fine. Just say so in a straightforward and explicit way. And then explain to us why you felt it was important to bomb this website with stuff about heterogeneous HIT that everyone already knew. No one has ever said that studies about heterogenous HIT aren’t important if you’re an epidemiologist. Issues about heterogeneous HIT have been around for decades going back to at least the 1920s when the first homogeneous HIT model was developed. The relevant issue is whether or not heterogeneous HIT models should inform any responsible policy debate. Policies that implement heterogeneous HIT theories are probably immoral even if they turn out to be scientifically valid. They are probably immoral for what I hope are obvious reasons.
I don’t know how you limited the Paul/Fauci discussion to: ” they were talking about various studies that have been looking at cross-reactivity immunity with other coronaviruses.”
Because you’re the one who said Sen. Paul was referring to a heterogeneous HIT study. He wasn’t. The exchange between Paul and Fauci was about something completely different:
Paul cut off Fauci, dismissing those mitigation efforts. He implied instead that New Yorkers have “developed enough community immunity” to beat the pandemic.
“I challenge that,” Fauci said. “You were not listening to what the director of the CDC said, that in New York, it’s about 22 percent. If you believe 22 percent is herd immunity, I believe you’re alone in that.”
Herd immunity occurs when enough people become immune to a contagious disease, making further spread unlikely. Those trained in infectious disease say at least 60 percent of a population needs to have been exposed to a virus to reach herd immunity.
But Paul referred to research suggesting people have “pre-existing, cross-reactive immunity to coronavirus,” which “may explain why we have so many people that have very little symptoms or are asymptomatic.”
Because most of us have been exposed to other coronaviruses, such as those that cause the common cold, our immune systems may already be trained to recognize SARS-CoV-2, the coronavirus that causes Covid-19.
There has been some research to back the theory cited by Paul, including one study that found immune cells called T cells could indeed account for the wide range of severity of Covid-19 symptoms.
However, Fauci responded by citing a recent study that found no evidence of pre-existing immunity from other coronaviruses.
https://www.nbcnews.com/health/health-news/fauci-paul-clash-over-covid-19-herd-immunity-senate-hearing-n1240858
Understand now? My suspicion is that you either got the Fox News version of the Paul/Fauci exchange or that you were completely confused and thought Paul was referring to heterogeneous HIT, but you’re just too proud to admit that you got things all confused. Anyway, I hope I’ve enlightened you and you won’t be inserting yourself into topics about which you know absolutely nothing.
2slugs, I will not follow you down your road of straw. If you want to talk policy, then talk to to policy makers.
“Because you’re the one who said Sen. Paul was referring to a heterogeneous HIT study.” No! See below. You also failed to answer: “I don’t know how you limited the Paul/Fauci discussion to: ” they were talking about various studies that have been looking at cross-reactivity immunity with other coronaviruses.”
I responded to his Fauci claim only: “You were not listening to what the director of the CDC said, that in New York, it’s about 22 percent. If you believe 22 percent is herd immunity, I believe you’re alone in that.” References say otherwise.
The remainder of your comment confuses terms so badly it is unreadable. Asymptomatic, presymptomatic or pre-symptomatic , Herd Immunity and your own use of HIT are all used either by you or our NBC News reference. The NBC reporter(s) were obviously not scientifically versed. When you follow their linkis you get to 2 studies. The 1st study was replete with some huge caveats. It also used a relatively high RT-PCR cycle rate for detecting Corona-Virus infections. Your reliance on that source and not noticing the glaring errors explains your own lack of scientific background in this area.
I noticed you also chose to ignore this reference in the NBC article “There has been some research (https://www.nih.gov/news-events/nih-research-matters/immune-cells-common-cold-may-recognize-sars-cov-2)to back the theory cited by Paul, including one study that found immune cells called T cells could indeed account for the wide range of severity of Covid-19 symptoms.”
Clearly, I’m not interested in discussing policy GENERAL guidance. Every time I follow up a specific claim iI find t is false.
2slugs, if you notice, corev does not even know what he is arguing about. his entire goal is simply to create confusion around an issue. when he gets caught explicitly, he simply changes the course of the argument. of course there are others on this blog, like rick stryker, who are better at this game than corev. but corev tries anyways. corev still believes that asymptomatic response is a result of herd immunity. difficult to argue with an idiot.
baffling Right. He’s trying to pretend that I was making a different point. He thought Sen. Rand Paul was talking about heterogeneous HIT when Sen. Paul was actually talking about cross-reactive herd immunity. Also, notice that he still hasn’t answered my question as to why he thinks a theoretical HIT of 22% implies policy decisions that are any different from a 60% HIT. In one post he told us that we couldn’t wait for the results of a long term study due to the urgency of the pandemic. If that’s so, then there must be some policy implications that we’re not pursuing in the absence of resolving the issue quickly.
CoRev is a very proud old man who cannot accept the fact that he’s wrong about so many issues. This is a guy who not only voted for Richard Nixon twice, but still believes the Iraq War was a great idea. For all I know he still believes Saddam’s nuclear weapons are still out there waiting to be found.
Baffled, you may have guessed I was referring to you about false claims.
2slugs, in the later thread you finally admit that we were talking ALL ALONG about Re. Your have been wrong from the begging due to your unwillingness to actually read the literature. When you did you realized that Re. Did some of your R calculations.
The next step is to evaluate/anasyze those SPECIFIC policies you so desperately want to discuss.
Making this statement indicates at this writing you were still in the desert re the HIT discussion: “…theoretical HIT of 22% implies policy decisions that are any different from a 60% HIT. In one post he told us that we couldn’t wait for the results of a long term study due to the urgency of the pandemic.” No, not theoretical, but calculated from a set of assumptions discussing the heterogeneity of the “herd”. From wiki: “Effective reproduction number
In reality, varying proportions of the population are immune to any given disease at any given time…” Just one of those heterogeneous assumptions needed to do the Re calculation, along with those policies you wish to discuss.
Your ego colored your thinking so badly you couldn’t see the obvious errors of comparing the policy differences between your R0 60% versus the Re 22% numbers.
For G$$s sake get over your arrogance. I don’t want to clean the coffee off my computer again.
the more you read of corev and his incoherent comments, the more you wonder if somebody should call 911 for him. it is like we are having a ron paul moment…
CoRev is aflame with all sorts of gibberish of late but this one takes the cake:
“CoRev
September 26, 2020 at 5:18 am
Baffled, there you go again arguing something while missing the sarcasm of consensus science. I guess in your world there can never, never, ever be a scientific breakthrough by an individual or minority of scientists. SCIENCE ONLY OCCURS BY THE MAJORITY (CONSENSUS)!”
What prompted this? Oh yea Rand Paul spouting some herd immunity crap not seemingly back by any science. Now CoRev reaches to the bottom of the barrel to find some non-peer reviewed paper that does not exactly support Paul’s cracked up thesis, which of course CoRev thinks is a “scientific breakthrough”. I guess this utter moron does not get that if a potential treatment shows any promise at all, other scientists will test it for efficacy and safety. Two words that CoRev clearly have never grasped.
Next up CoRev will be promoting blood leaching as a cure for Coronavirus.
I think I have found CoRev’s Coronavirus expert. Professor Marvel from the Wizard of Oz:
https://www.youtube.com/watch?v=PJaxd1BQr9g