The Golden Rule: Understand…your…data
[Updated to incorporate 6/9/2020 data] A commenter on twitter writes:
Here’s the real data straight from the WI DHS website. Trend is down no matter how much you want it to be going higher. https://dhs.wisconsin.gov/covid-19/county.htm

Is this assertion true? Are deaths really falling drastically, if we look at deaths by date of occurrence. Unfortunately, an important caution in the notes was ignored:
This chart is called a mortality curve. It is used to track the number of deaths over time and see when peaks occur. This figure is showing data by when a person died. Date of death is more meaningful than using the date when the person’s death was reported to public health.
When presenting data by the date of death, any downward trends that are seen during the most recent two weeks are usually not true decreases in deaths and need to be interpreted with caution. This downward trend usually represents the data lag time; thus, data during the most recent two weeks are highlighted as preliminary data. It takes time for patient deaths to be reported to public health and to be included in death counts.
There are two ways to see the hazards of ignoring this warning. First, examine the revisions; second, examine the two cumulative series for the “death-by-date” and “death-by-date-of-report”.
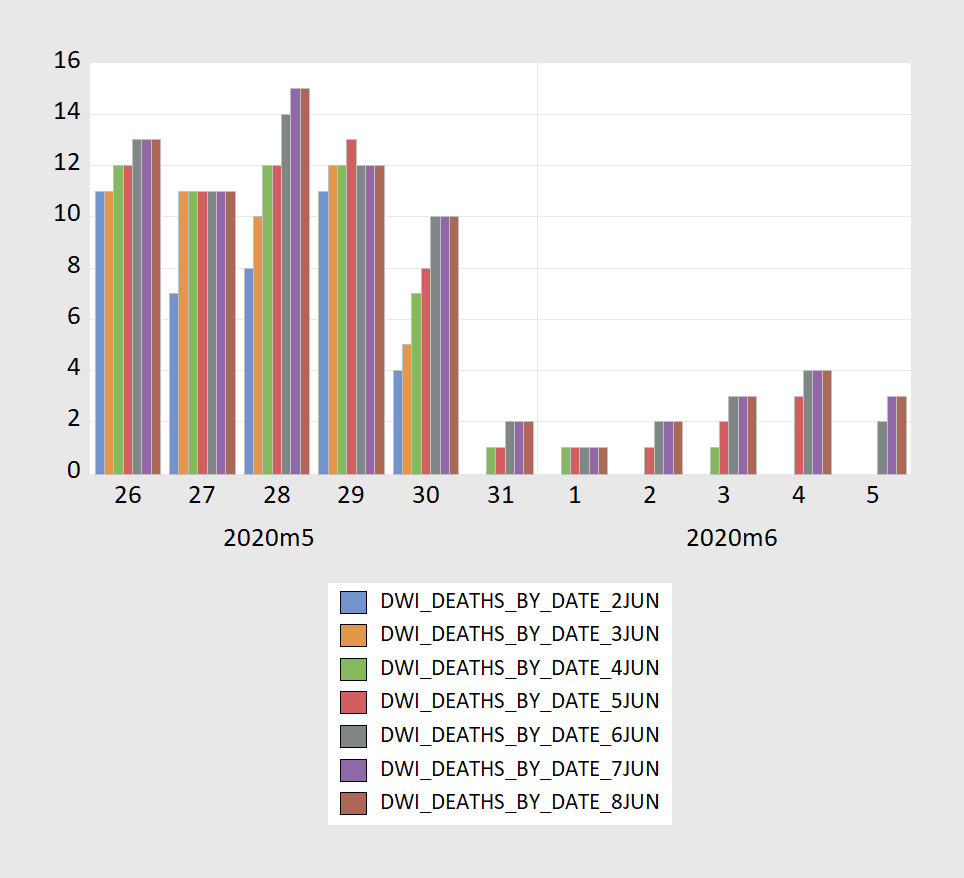
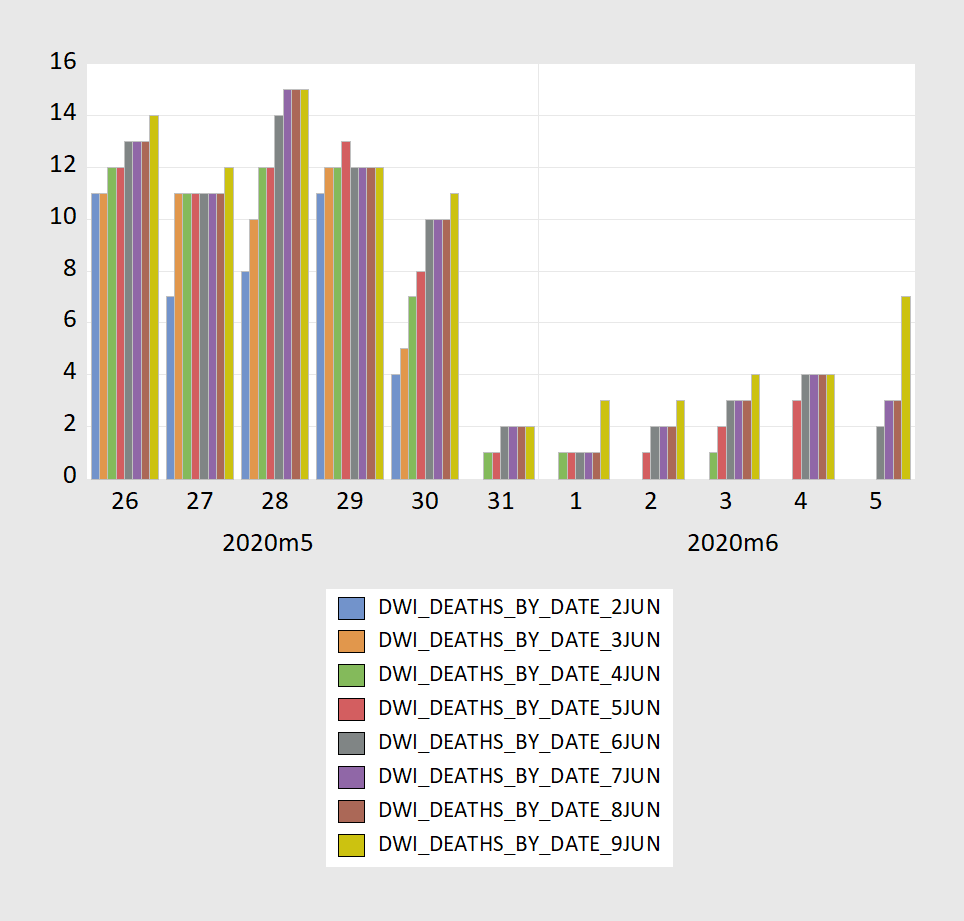
Figure 1: [Updated] Wisconsin Covid-19 deaths-by-date, according to June 2 vintage (blue bar), according to June 3 vintage (tan bar), according to June 4 vintage (green bar), according to June 5 vintage (red bar), according to June 6 vintage (gray bar), according to June 7 vintage (purple bar), according to June 8 vintage (brown bar) and according to June 9 vintage (chartreuse bar). Source: Wisconsin Department of Health Services.
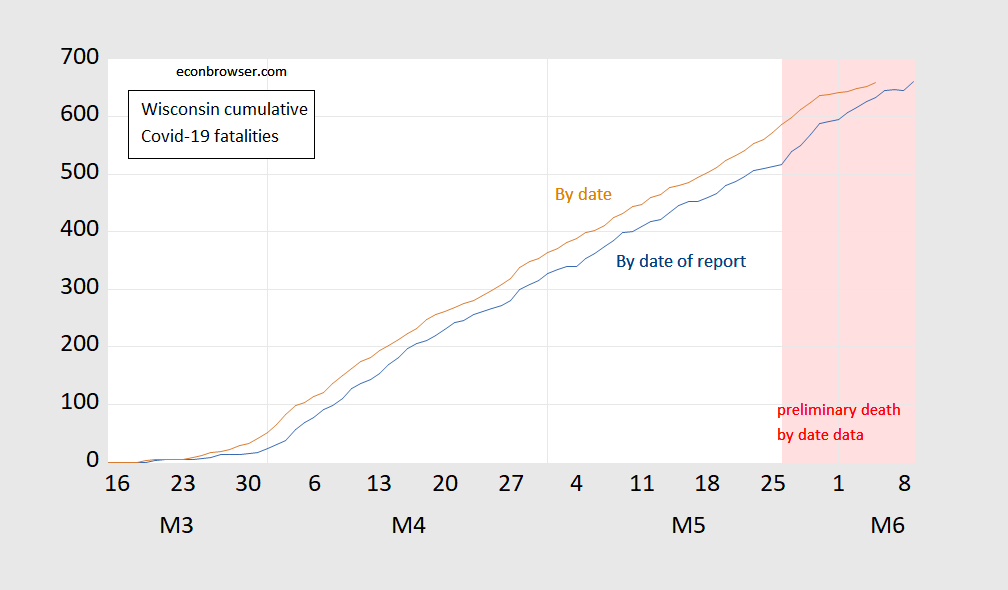
Figure 2: [Updated] Wisconsin Covid-19 cumulative fatalities by date reported (blue), and by date of death (tan). Light pink shaded area denotes data that is denoted “preliminary” by WI DHS as of 9 June 2020. Source: Deaprtment of Health Services [1], [2], and author’s calculations.
Notice that over time, deaths-by-date change (rise) as new data come in over time — hence the caveat on the DHS website (twice!). Figure 2 shows that over time cumulative deaths-by-date catch up with cumulative deaths as recorded- but generally lags, and as Figure 1 shows, lags the most in the most recent data at any given time. Hence, to repeat for those who are unable to read:
When presenting data by the date of death, any downward trends that are seen during the most recent two weeks are usually not true decreases in deaths and need to be interpreted with caution.
Now, it might be the case that in the past week, Covid-19 fatalities by date have declined — but I would be hard pressed to honestly make such a judgment.
In general, those who wish to do data analysis in real time need to resist the temptation to rush and download the data, and need to read the data description. That’s the first rule I give my students in stats-for-policy course. Easy enough to remember and implement in the old days when you had to transcribe the data by hand from hard copy to type into the computer. Hard these days when you can click and download…
(For other disasters in data analysis in real time using subject-to-revision administrative data, see here.)
The CDC did an interesting analysis that strongly implies risk by age. It’s interesting to note that people under 25 are at extremely low risk and the closing of schools and universities is probably the ultimate case of overkill reaction to a disease. https://data.cdc.gov/NCHS/Provisional-COVID-19-Death-Counts-by-Sex-Age-and-S/9bhg-hcku
It’s also interesting to look at the number of deaths and implied risks from influenze and pneumonia for younger people.
Yes, the numbers have been affected by all sorts of factors, so I’ll admit they are not “clean” in the sense of perfect, but they are strongly directional.
As far as Wisconsin is concerned, look at the population changes between 2010 and 2014 by age group: https://www.dhs.wisconsin.gov/population/wisconsin2014.pdf
Wisconsin is becoming a geriatric state and at increased risk for Covid-19 deaths as a result. Keep your old folks out of nursing homes.
Bruce Hall You might have a point if we can figure out a way to keep school age children from coming in contact with their parents and grandparents and their teachers, most of whom are likely to be older than 25. Similar story with college students coming in contact with their professors, all of whom will be older than 25. And death isn’t the only bad outcome. Suppose you’re a college student who plunks down 10 or 20 grand for a semester and then comes down with COVID-19 in mid-November. You’ve not only lost a semester’s worth of credits, but you’re out 10 or 20 grand. The best you could hope for is a sympathetic professor who would be willing to give you an incomplete. In pre-COVID days that sort of thing would happen, but it was fairly rare. But in a COVID-19 world it would be fairly common. Just because the mortality rate for twentysomethings isn’t high doesn’t mean the effects aren’t debilitating.
BTW, Sweden’s chief heath official who was responsible for Sweden’s “herd immunity” approach recently admitted that he was wrong and Sweden should not have gone down that route. I’ll give him credit for at least owning up to his mistakes…unlike some of our politicians.
Median retirement age 2018-2019 for K-12 teachers in California (according to CalSTRS) was 62.9.
France and Israel may disagree. They reopened kids passed it all over the place.
“and the closing of schools and universities is probably the ultimate case of overkill reaction to a disease. ”
Nonsensical argument. If you have a lot of cases in the population, closing schools is one of the most effective step to bring them down. High quality papers on this issue are dicussed by Prof. Drosten in his podcast.
“the closing of schools and universities is probably the ultimate case of overkill reaction to a disease.”
So when the kids come home they do not interact with adults? Now we know when the kids see you they run and hide but you are not the only old person in your town.
@Bruce Hall – your post about those under 25 is akin to cherry picking incomplete data. I suggest you go to my COVID-19 site and start getting some education about what is and isn’t true about this virus: https://agoldhammer.com/covid_19/ Since my daily newsletter is free, I’ll be happy to add you to the subscription list!!! I have always been in favor of prudent reopening of the country once the hospital crises was ended. Unfortunately, a number of states have not gotten the message and are opening without any plan in place. Arizona just sent out a health alert about ICUs nearing capacity because of spikes. The health commissioner of Orange County CA was forced to resign as she did want her house picketed and young children threatened by anti-maskers. We are going to see COVID-19 infections continue to run at a higher level than they need to because so many people don’t understand simple public health. It is just too sad to see this continue.
If private bone spurs would quit hiding in his bunker and step out and lead, he could advise the country of the dangers of going without masks. The antivaxers will form the next battleground. Alas, all that i expect from bunker don is continued silence broken with an occasional conspiracy or racist tweet.
Bruce Hall Keep your old folks out of nursing homes.
So unless you’re fabulously wealthy, that generally means having the “old folks” move in with their kids…and oh yes, grandkids. So apparently you’re recommending that kids go to school so they can infect their grandparents at home. Is that what you’re suggesting? You really need to think about what you post before you hit the keyboard.
As to influenza and pneumonia risks, we do have vaccines and proven therapies for those.
2slugbaits: I think that is his recommendation, so as to better reduce the surplus population…Didn’t you ever watch “Logan’s Run” (although book was better).
Keep the old folks out of the nursing homes and at home, where the grandkids can Spread the disease they caught from school. You are an idiot bruce.
Or, in the alterative right wing world of paid trolls –
The Golden Rule: misrepresent…your…data
Many are assuming that death is the only long term effect of the disease. This assumption leads many to conclude that if death rates are low for a group then total risk is also low. This conclusion is faulty given our lack of knowledge, although it may be years or decades before we truly know the long term effects for survivors.
If it does attack vascular systems as the current thinking holds, then the true damage may not show up for a decade or more. Those in their 20s may have severe health problems in their 30s or 40s or later due to an infection. They may not. We don’t know, but the virus does enough weird things that nothing can be ruled out for now. That’s not being paranoid, that’s being observant.
All the more reason to cut overhead from health insurance premiums. Hundreds of thousands of people may need more medical care in the future than would have been the case without the pandemic. Private health insurance has far higher overhead than publicly provided health insurance.
Life insurance premia are also likely to rise, given the risk of early death due to Covid-induced damage.
As to Bruce’s analytical lapse – wow, that was a big one.
Jay Exactly. One way to look at is to ask folks like Bruce Hall how much they would have to be paid in order to be infected with COVID-19 even with a 100% guarantee of not dying. I seriously doubt that he would settle for $0. He would want some kind of compensation for the pain (in some cases downright agony) that accompanies a significant portion of COVID-19 recoveries.
Apparently Harold Uhlig and Rick Stryker share the same worldview-black people should stay in their lane and quit complaining.
https://www.cnbc.com/2020/06/11/yellen-joins-chorus-against-economist-who-criticized-black-lives-matter.html
it is folks like harold who give economists a poor public reflection during difficult times. kind of like the economists who still insist corporations should act solely in the name of maximized profits.